Article Text

Abstract
Introduction Strong primary health care (PHC) leads to better health outcomes, improves health equity and accelerates progress towards universal health coverage (UHC). The Astana Declaration on PHC emphasised the importance of quality care to achieve UHC. A comprehensive understanding of the quality paradigm of PHC is critical, yet it remains elusive in countries of the Eastern Mediterranean Region (EMR). This study used a multistep approach to generate a policy-relevant research agenda for strengthening quality, safety and performance management in PHC in the EMR.
Methods A multistep approach was adopted, encompassing the following steps: scoping review and generation of evidence and gap maps, validation and ranking exercises, and development of an approach for research implementation. We followed Joanna Briggs Institute guidelines for conducting scoping reviews and a method review of the literature to build the evidence and gap maps. For the validation and ranking exercises, we purposively sampled 55 high-level policy-makers and stakeholders from selected EMR countries. We used explicit multicriteria for ranking the research questions emerging from the gap maps. The approach for research implementation was adapted from the literature and subsequently tailored to address the top ranked research question.
Results The evidence and gap maps revealed limited production of research evidence in the area of quality, safety and performance management in PHC by country and by topic. The priority setting exercises generated a ranked list of 34 policy-relevant research questions addressing quality, safety and performance management in PHC in the EMR. The proposed research implementation plan involves collaborative knowledge generation with policy-makers along with knowledge translation and impact assessment.
Conclusion Study findings can help inform and direct future plans to generate, disseminate and use research evidence to enhance quality, safety and performance management in PHC in EMR and beyond. Study methodology can help bridge the gap between research and policy-making.
- primary healthcare
- quality of care
- patient safety
- performance management
- scooping review
- evidence and gap map
- priority setting
- knowledge translation
- research implementation
- health policy and systems
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- primary healthcare
- quality of care
- patient safety
- performance management
- scooping review
- evidence and gap map
- priority setting
- knowledge translation
- research implementation
- health policy and systems
Key questions
What is already known?
There is a gap in knowledge and a need to prioritise research in the area of quality, safety and performance management in primary health care (PHC) in the Eastern Mediterranean Region (EMR).
What are the new findings?
This is the first study to use a multistep approach to generate a policy-relevant research agenda to strengthen quality, safety and performance management in PHC in the EMR.
The resultant evidence and gap maps provide an overview of research evidence and gaps by country, study design and dimensions of quality, safety and performance management.
The top five research priorities for quality, safety and performance management in PHC in the EMR for the next 3–5 years are identified.
What do the new findings imply?
Study findings can help bridge the gap between research and policy, and contribute to the development of evidence-informed policies and practices in PHC in the EMR and beyond.
Researchers, funding agencies and countries can support and align human and financial resources towards addressing the research priorities that have been identified.
Introduction
The Alma-Ata Declaration envisioned primary health care (PHC) as an integral part of a country’s health system and of the overall social and economic development of the community.1 Strong and comprehensive PHC leads to better health outcomes, improves health equity, reduces inefficiencies of health systems and accelerates achievement of the health-related sustainable development goals (SDGs) including the transformative aim of universal health coverage (UHC).2–5 The UHC target of the SDGs specifies that everyone should have access to essential health services at high quality without suffering financial hardship; yet, the quality dimension of care has not been widely tracked.6 7 The recent Astana Declaration on Primary Health Care has brought the issue of quality to the forefront of discussions, emphasising the need to develop quality primary care that is continuous, comprehensive, coordinated, community-oriented and people-centred in order to achieve the UHC goal of SDGs.8
Worldwide, governments have been urged to prioritise PHC services to achieve care that is relevant, equitable, high quality and cost-effective.9–11 Nonetheless, PHC remains undervalued in many parts of the world, particularly in low-income and middle-income countries (LMICs) where most of the investments are being channelled towards acute hospital care.12 13 Where efforts have been made, these have mainly focused on increasing coverage of essential health services, aided by global initiatives to measure and compare coverage across countries, with less efforts invested in improving the quality and safety of services in PHC.14 15
Eastern Mediterranean Region
The importance of PHC in the Eastern Mediterranean Region (EMR) has been emphasised through a resolution that called upon member states to set up delivery models for primary care services, increase allocation of resources to primary care and ensure availability of adequately distributed human resources for PHC.16 While several, although fragmented, initiatives are being undertaken to strengthen PHC in countries of the EMR,17 the multidimensional nature of quality necessitates assessment and calibration at different levels and targeting different players and stakeholders.18–20
A review of the literature on quality of care in PHC covering the period 2000–2012, concluded that the process dimension of quality, specifically clinical practice and patient–provider relationship, is an area of major concern.18 Some of the factors contributing to suboptimal quality, safety and performance management in PHC include the absence of a clear vision and strategic direction to guide and support the implementation of quality and safety interventions, weak public/private collaboration, misdiagnosis, prescription and medication errors and absence of institutionalisation of quality and safety.17 21–23 This is further exacerbated by the increasingly complex challenges facing the EMR countries including demographic and epidemiological transitions, massive migrations and population displacements, limited financial support to health systems and poor referral systems.24 25
A comprehensive understanding of the quality paradigm of PHC is critical, yet it remains elusive in countries of the EMR. Moreover, the need to prioritise research in the area of quality and safety has been reiterated by policy-makers and stakeholders in several regional meetings.17 26 Eliciting policy-makers’ priorities and aligning research production with those priorities can increase the likelihood of research uptake into policy and practice.27 28 Therefore, this study aimed to generate a policy-relevant research agenda for strengthening quality, safety and performance management in PHC in the EMR. The specific objectives of the study were to: (1) provide an overview of research evidence and gaps pertaining to quality, safety and performance management in PHC in the EMR; (2) generate and rank research questions addressing the research gaps; and (3) propose an approach to promote the uptake of research into policy and practice.
Methods
A multistep approach was adopted, encompassing the below steps which correspond to the different objectives of the study:
Step 1: Scoping review and generation of evidence and gap maps (objective 1).
Step 2: Priority setting meeting with policy-makers and stakeholders (objective 2).
Step 3: Proposed approach for research implementation (objective 3).
Patient and public involvement
Patients and the general public are involved in steps 2 and 3 of the multistep approach. Specifically, they were involved in the validation and ranking of research questions through the non-governmental organisations that participated in the priority setting meetings (step 2). They are also included in the different steps of the proposed approach for research implementation addressing the top ranked priority question (step 3).
Step 1: scoping review and generation of evidence and gap maps
Study design
We conducted a scoping review to identify and map the research evidence on quality, safety and performance management in PHC in the EMR. A scoping review is typically used to present ‘a broad overview of the evidence pertaining to a topic, irrespective of study quality, to examine areas that are emerging, to clarify key concepts and to identify gaps’. We followed the Joanna Briggs Institute (JBI) guidelines for conducting and reporting scoping reviews.29 We also followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Extension checklist for reporting scoping reviews.30 Similarly, for developing the evidence gap map, we relied on the results of a methodological review on these maps.31
The scoping review aimed to achieve the following:
Provide a comprehensive overview of where the research evidence exists and where there are major gaps, irrespective of study design, when it comes to quality, safety and performance management in PHC in the EMR.
Examine the subset of effectiveness studies related to quality, safety and performance management in PHC in the EMR, with a focus on the interventions used and the outcomes measured.
Conceptual framework
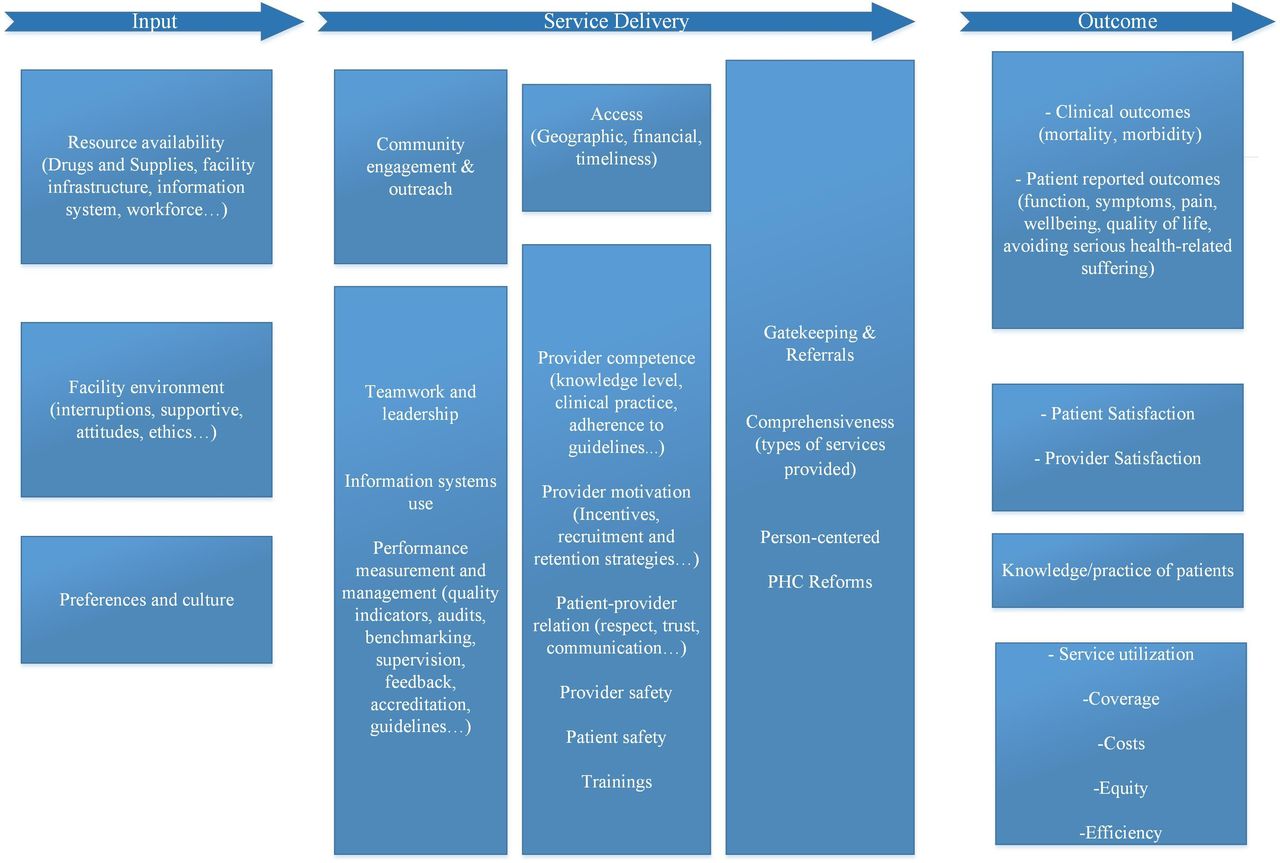
The conceptual framework for this study was adapted from the Primary Health Care Performance Initiative (PHCPI) (figure 1). We used the PHCPI framework as a starting point for conceptualising this research as it covers all the necessary components of high-functioning PHC systems.32 However, given that the framework focused on the entirety of PHC, and the scoping review is oriented towards quality, safety and performance management, we subsequently refined it in order to make it more focused on quality, safety and performance management issues.

Conceptual framework for quality, safety and performance management in primary healthcare (PHC).
The revised framework encompasses the following three dimensions: (a) inputs (characteristics of the settings in which care is provided including organisational structure, material resources and human resources); (b) service delivery (activities related to provision of care including diagnosis, treatment and patient interactions with the healthcare structure); and (c) outcomes (effects of care on health and health system outcomes) (figure 1). The inputs affect service delivery and outcomes, and the outcomes reflect the combined effects of inputs and service delivery. The operational definitions for the different themes under each dimension have been adapted from PHCPI framework and are presented in online supplementary file 1.
Supplemental material
Eligibility criteria
Study design: We included all study designs except letters, correspondence, commentaries, dissertations, technical papers, handbooks, protocols and editorials.
Setting: We included studies that focused on countries of the EMR (ie, Algeria, Bahrain, Comoros, Djibouti, Egypt, Iraq, Iran, Jordan, Kuwait, Lebanon, Libya, Mauritania, Morocco, Oman, Palestine, Qatar, Saudi Arabia, Somalia, Sudan, Syria, Tunisia, United Arab Emirates and Yemen). For a study to be included, it should focus on PHC, outpatient clinics, family medicine departments and/or community settings.
We excluded studies that focused on the health system in general without segregating findings for PHC. Additionally, we excluded studies that took place in hospitals or university settings; for example, studies assessing the knowledge, attitudes and practices of residents or medical students.
Population: We did not limit the search to any specific type of population.
Dimensions and themes of interest: We included studies that focused on any of the dimensions and/or themes pertaining to quality, safety and performance management as depicted in the framework (figure 1). Moreover, those dimensions and/or themes should be reflected in the objectives and results section of a study as opposed to only in the background section.
We excluded studies that assessed the prevalence of a specific condition or disease at the population level without linking it to any of the dimensions depicted in the framework. We also excluded studies that sampled patients from PHC for other purposes beyond the aim of this scoping review. Additionally, we excluded studies that assessed the lifestyle behaviour of physicians, for example, smoking or drinking habits without linking it to quality, safety or performance management in PHC.
We did not restrict the search to any language or date.
Literature search
We searched the following electronic databases between February and March 2018: MEDLINE, CINAHL, HSE and PubMed. We used both index terms and free text words for the following three concepts: (1) PHC; (2) quality, safety, performance management; and (3) EMR. The search terms and MeSH terms for each database were developed and validated with the guidance of an information specialist (see online supplementary file 2 for full search strategy).
Supplemental material
Selection process
Prior to proceeding with the selection process, we conducted a calibration exercise to enhance validity of the selection process. We completed the selection process in two stages:
Title and abstract screening: Teams of two reviewers used the above eligibility criteria to screen titles and abstracts of identified citations in duplicate and independently for potential eligibility. We obtained the full text for citations judged as potentially eligible by at least one of the two reviewers.
Full-text screening: Teams of two reviewers used the above eligibility criteria to screen the full texts in duplicate and independently. They resolved disagreement by discussion or with the help of a third reviewer. They used standardised and pilot tested screening forms.
Data abstraction
Teams of two reviewers abstracted data from each study using standardised and pilot-tested forms. Any disagreement between the reviewers was resolved by discussion, and when needed, with the help of a third reviewer. We conducted calibration exercises to ensure the validity of the data abstraction process.
We abstracted the following information from all included studies:
Citation.
Year of publication.
Country of affiliation of contact author.
Country of affiliation of first author.
Study design (systematic/scoping review, randomised trial, cohort, quasi-experimental, chart/document review, qualitative, literature review, mixed methods).
Language of publication.
Country in which the study was conducted.
Focus of the study as it relates to the dimensions and themes in the framework.
For the subset of studies examining the effectiveness of interventions (ie, effectiveness studies), we also abstracted the following additional information:
Intervention: provider-targeted interventions, patient-targeted interventions, organisational/systems level interventions and multifaceted interventions.
Outcome: provider outcomes, patient outcomes, organisational outcomes and systems outcomes.
Risk of bias assessment
We did not perform appraisal for risk of bias since this is a scoping review, consistent with the JBI guidelines.29
Data analysis
The main focus of the studies were ‘charted’ using the dimensions and respective themes depicted in the framework.33 Data coding involved three phases: deduction (coding data and labelling each section), induction (screening data for new concepts or codes to emerge) and verification (verifying all coded data).34
For the deduction phase, we used the modified PHCPI framework as a starting point for the selection of themes under each dimension; we also leveraged the findings of a systematic review on quality and safety in PHC to refine the themes.35 Additionally, for effectiveness studies, we used the findings of a systematic review of strategies for improving quality and safety of healthcare, to generate a list of coding themes for interventions and outcomes, respectively.36 For the induction phase, the reviewers screened the ‘result’ section of each study and coded the findings against the predefined themes, while also allowing for new themes to emerge inductively. We iteratively updated the coding themes as we proceeded with data analysis. Throughout the process, all team members were consulted to validate coding decisions and discuss emerging themes. We revisited and considered data in the context of any newly emergent theme.
The revised lists of coding themes are presented in online supplementary files 3.
Supplemental material
Data synthesis
Findings were synthesised quantitatively (using frequencies) and qualitatively (thematic analysis).
We used the results of the scoping review to construct evidence and gap maps on quality, safety and performance management in PHC in the EMR. A gap map is defined as ‘a systematic search of a broad field to identify gaps in knowledge and/or future research needs’. These maps present results in user-friendly formats such as cross-tables, visual figures or graphs or a searchable database.31
Two evidence and gap maps were constructed: (1) a main map focusing on the different dimensions and themes pertaining to quality, safety and performance management, and encompassing all types of study designs; and (2) a submap focusing specifically on interventions and strategies addressing quality, safety and performance management, and thus, encompassing only effectiveness study designs. The conceptual framework depicted in figure 1 was used to guide the construction of the main map. For the submap, the list of coding themes in online supplementary file 3 was used to guide the process.
Step 2: priority setting meeting with policy-makers and stakeholders
Generation of potential research questions
An initial list of research questions was generated addressing the research gaps identified from the evidence and gap maps. This list was subsequently revised by removing duplicates and merging overlapping questions.
To arrive at well-formulated and focused research priorities, we adopted the following criteria for question generation: (1) answerable through a realistic research design, (2) has a factual answer that does not depend on value judgements, (3) addresses important gaps in knowledge, (4) not formulated as a general topic area, (5) not answerable by yes or no and (6) if related to impact and interventions, contains a subject, an intervention and a measurable outcome. The questions were iteratively refined based on ongoing consultations and discussions with core team members throughout this step.
Validation and ranking of research questions
Four priority setting meetings were conducted in selected countries of the region—Lebanon, Jordan, Tunisia and Bahrain—to validate and rank the list of research questions generated from the evidence and gap maps. These countries were purposively selected based on their income classification and in consultation with members of the core team. The selection was also influenced by feasibility, budgetary and time constraints.
To assist with coordination of the priority setting meetings, a local researcher was identified from each country. The choice of local researcher was guided by defined criteria including previous experience in undertaking health systems research, good knowledge of policy-making process and potential to access relevant key informants. Once selected, the local researchers helped in recruiting key country-specific informants, based on the below sampling framework37:
Policy-makers from the public sector such as officials from ministries of health.
Representatives from professional associations of relevance to PHC.
PHC directors/managers.
Academia/researcher.
Representatives of non-governmental organisations.
Healthcare quality experts.
Each priority setting meeting involved a small diverse group of 10–18 individuals purposively selected from each country based on the above sampling framework. Members from the core research team and the local researcher co-facilitated the meetings in Lebanon, Jordan and Bahrain, respectively. As for Tunisia, the local researcher facilitated the meeting, with clear detailed guidance provided by the core research team prior to the meeting. The priority setting meetings served the following two purposes1: validate the list of research questions related to quality, safety and performance management in PHC (generated from the gap map); and2 subsequently rank the validated questions against a set of specific criteria.
A standardised survey tool was developed and distributed to participants for ranking of questions (online supplementary file 4). The ranking criteria were derived from a previous priority setting exercise conducted in the region37 and complemented by additional criteria extracted from SPARK tool.38 Each research question was ranked against the below set of criteria, on a 3-Likert scale (low, medium and high):
Supplemental material
Relevance: Is this question relevant to policy/community concerns?
Urgency: Is the evidence on this question needed within the next 1–3 years?
Feasibility: Is this research question do-able in your country?
Applicability: Once we have evidence on this question, can it drive policy changes?
Impact on health: will addressing this question lead to improvements in health outcomes?
The surveys were filled on anonymous basis by each participant and subsequently returned to the core research team. Data were analysed using SPSS V.25. Equal weight was given to all criteria and therefore total scores in addition to means and SD were computed for each research question. The research questions with the highest mean scores were designated as the top priority questions.
Step 3: proposed approach for research implementation
Acknowledging that priority setting is just a first step in the knowledge spectrum, and that the production of research does not, on its own, lead to widespread implementation or effect on health outcomes,39 we adapted the impact-oriented approach by El-Jardali and Fadlallah to promote impactful research that can enhance quality, safety and performance management in PHC.21 The impact-oriented approach is a generic approach that can be applied to any research question to help promote the uptake of research results into health policies and practices. The approach encompasses all steps from priority setting to research production, knowledge translation and impact assessment. A key emphasis is on the need to link production of research addressing a priority question, to knowledge translation activities that facilitate use of research to inform decisions and changes in policy or practice. The entire process is iterative and driven by the desired end results.
The research question with the highest mean score was designated as the top priority question to be addressed in the research implementation plan. The proposed approach was subsequently tailored to the top ranked priority question. We also relied on the literature to inform the research methodology for that specific question.
Results
The Results section is divided into the following three parts, reflecting the different study objectives:
Scoping review and evidence and gap maps.
Priority research questions.
Proposed approach for research implementation.
Scoping review and evidence and gap maps
Study selection
Online supplementary file 5 shows the PRISMA flow chart summarising the study selection process. Of the 6095 citations identified, 484 studies met the eligibility criteria. At the full text screening, we excluded 544 articles for the following reasons: not region of interest (n=51), not setting of interest (n=236), not design of interest (n=52), not topic of interest (n=153) and others (n=52) (see online supplementary file 6 for details).
Supplemental material
Supplemental material
Characteristics of included studies
Table 1 provides an overview of the characteristics of the included studies. Full details of study characteristics can be found in online supplementary file 7.
Supplemental material
General characteristics of included studies (N=484)
The studies were published between the years 1981 and 2018 (inclusive) and were conducted in 19 countries of the EMR. The majority of the studies were conducted in Saudi Arabia (n=143; 29.5%) followed by Iran (n=65; 13.4%) and Jordan (n=35; 7.2%), and 87% and 82.6% of first authors and corresponding authors, respectively, were affiliated with institutions from EMR countries. The majority of studies were published in English language (n=463; 95.7%).
The resultant evidence and gap maps provide an overview of available evidence and gap by country, study design and dimensions of quality, safety and performance management, while also specifying the number of studies. Online supplementary file 8 provides links to the interactive evidence and gap maps.
Supplemental material
Main map (N=484)
The main evidence and gap map provide a visual overview of the entire evidence base, stratified by country, study design and dimensions of quality, safety and performance management (figure 2 and online supplementary file 8). The majority of studies were conducted in Saudi Arabia followed by Iran, Jordan, Egypt, Bahrain and Lebanon. No primary studies were identified for the following five countries: Comoros, Djibouti, Libya, Mauritania and Somalia.

Main map: dimensions of quality, safety and performance management in primary healthcare in Eastern Mediterranean Region (EMR) (N=484).
Most of the study designs were descriptive/cross-sectional (n=273; 56.4%), followed by chart/document reviews (n=63; 13%). Twenty-four studies (or 5%) used an experimental or quasi-experimental study design. Only two systematic reviews were identified, one focusing on the EMR and another focusing on Iran.18 40
The highest proportion of articles examined the ‘service delivery’ dimension (n=446; 92.1%), followed by the ‘outcome’ dimension (n=219; 45.2%), with the least number of studies examining the ‘input’ dimension of quality (n=85; 17.6%). The major theme explored was ‘provider competency’ and was mainly studied in Saudi Arabia, Iran, Jordan and Bahrain. Providers were evaluated on diverse clinical and organisational topics such as management of diabetes mellitus and its associated complications, management of acute respiratory infections, smoking and oral health, knowledge of AIDS, knowledge of high-quality referral writing, medication prescribing pattern and attitudes towards evidence-based medicine.
Submap (N=61)
The submap focuses on effectiveness/intervention studies and provides a visual presentation of the findings, stratified by intervention, outcome and study design (see online supplementary file 8 for interactive submap). The coding details are provided in online supplementary file 9.
Supplemental material
Provider-targeted interventions (n=37) were the most frequently assessed interventions. The second most assessed interventions were at the organisational/systems level (n=18), with the majority of studies examining the effect of condition-specific management programme on provider competencies, access to services and clinical outcomes. Fewer studies tackled patient-targeted interventions (n=9), with public health education and promotion being the mostly examined intervention at this level. The remaining eight studies assessed the effect of multifaceted interventions on provider competence, patient satisfaction, clinical outcomes and process improvements. Interventions scarcely or not examined through these effectiveness study designs included educational outreach, community-based interventions, supervision, recruitment and retention strategies, audit and feedback, public scorecards, performance report and external accreditation.
The most commonly assessed outcome category was patient-level outcomes (n=45) followed by provider-level outcomes (n=40) and organisational-level outcomes (n=31), with the least number of studies assessing systems-level outcomes (n=19). The most reported outcome across categories was provider competency (n=36). None of the studies examined ‘safety’, ‘provider motivation’ or ‘equity’ as outcomes of interest whereas ‘access’, ‘referrals’ and ‘patient-centred’ outcomes were examined in only two studies.
Priority research questions
An initial list of 43 questions was generated from the evidence and gap maps. Removal of duplicates and merging of similar questions reduced the number to 34. Overall, 55 participants from four selected EMR countries (Jordan=18, Bahrain=13, Tunisia=14 and Lebanon=10) participated in the validation and ranking of research questions. Participants’ affiliations were as follows: policy-making institution (n=18), academic institution (n=12), non-governmental organisation (n=8), professional association (n=4), health professional (n=9) and healthcare quality expert (n=4) (see online supplementary file 10 for participants’ affiliations by country). Seven participants (four from Jordan and three from Lebanon) could not attend the meetings in person, and thus, completed an online version of the survey tool.
Supplemental material
Table 2 presents the overall ranking of research questions by policy-makers and stakeholders across study countries (online supplementary file 10 presents the individual ranking by country). The top five-ranked priority questions across countries were:
Ranked list of research questions across study countries
What are the minimum sets of standardised and applicable quality and patient safety indicators to monitor PHC performance at national and regional levels?
What risk and safety management approaches can be adopted to enhance patient safety in PHC?
What regulatory and administrative measures can be implemented to promote rational drug prescribing in PHC?
What strategies are effective in promoting equitable access to PHC among the most vulnerable population?
What are the most effective methods for training clinicians in quality improvement?
Proposed approach for research implementation
Figure 3 presents the proposed approach for research implementation. The top priority question to be addressed in the research implementation plan corresponds to the establishment of minimum sets of standardised and applicable quality and patient safety indicators to monitor PHC performance at national and regional levels.

{kind=link}
{kind=link}
{kind=link}
Proposed approach for research implementation.
Existing literature on this priority question reveals that, while LMICs and countries of the EMR put less emphasis on quality measurement, high-income countries such as USA, Europe and Australia invest significant resources in measuring the level and variation in quality and associations with health outcomes.7 41 In particular, quality and safety indicators are increasingly being implemented in PHC in these settings to improve quality of care and reduce variations in performance across healthcare organisations.42–46 The information required to develop quality indicators can be derived using systematic methods which combine scientific evidence with expert opinions.43 45 To help maximise effectiveness of quality indicators, it would be important to select indicators that are valid, reliable, acceptable, applicable and make use of existing data sources.44 45 It is also necessary to consider the purpose of the date generated. For instance, in Europe and Australia, quality indicators are increasingly linked to incentives and re-imbursement systems which directly reward improvements in quality as well as achievement of levels of quality.42 47 48 To facilitate transference of indicators between settings and countries, it would also be important to standardise data collection tools and reporting systems to ensure accurate data collection and benchmarking.46
Drawing on the existing literature, we suggest a multistep iterative process for the knowledge production phase of the proposed approach in order to establish a minimum set of standardised indicators for quality and patient safety in PHC. The main steps include a (1) literature review of international indicators and inventory of existing indicators in selected EMR countries to generate a preliminary list of indicators; (2) a series of consensus meetings with key stakeholders including policy-makers, researchers, health professionals and patients to select the indicators for inclusion; (3) development of procedure manuals to standardise data collection methods; (4) pilot-testing and subsequent refinement of indicator measurement tools; and (5) preliminary implementation.45 49 50 Selected EMR countries can consider harmonising a subset of regional indicators while also maintaining a national set of indicators tailored to their own contexts and needs. Linking incentives and reimbursement to specific indicators can be introduced at later stages once the capacity is built for collecting and reporting indicators. This will help ensure collection of sufficient and valid measurements that can enable reliable comparisons across settings and countries.
Following the knowledge production phase, knowledge translation activities will be undertaken to facilitate moving evidence into policy and practice.21 39 51 Knowledge translation products are characterised by their ability to simplify and support information exchange between research producers and research users in order to reach evidence-informed health decisions.52 A widely used knowledge translation product is Evidence Brief for Policy which synthesises research in a user-friendly format, taking into consideration global research evidence as well as context-specific research results to support well-informed policy decisions.53 Evidence Briefs for Policy are increasingly used as input into policy dialogues. Thus, following their preparation, national and regional policy dialogues will be convened with key stakeholders to inform deliberations about the question of interest and agree on next actionable steps.
Prospective health policy tracing will help assess the uptake of research evidence in policies and practice in study countries.54 Real-time lessons from the experiences of study countries (including facilitators, challenges and sustainability issues) will be drawn to help strengthen PHC in the EMR and beyond.
Discussion
To our knowledge, this is the first study to use a multistep approach to generate a policy-relevant research agenda in the area of quality, safety and performance management in PHC in the EMR. The study generated three important outputs: evidence and gap maps, a ranked list of priority research questions and a proposed approach for research implementation addressing the top-ranked priority question. Study outputs can help strengthen quality, safety and performance management in PHC in the EMR and beyond.
The evidence and gap maps revealed limited production of research evidence in the area of quality, safety and performance management in PHC by country and by topic. Scarcity of research in the EMR has been attributed to limited funding as well as lack of local capacity for conducting research.55 Despite the geographical diversity of the region, more than half of the studies were concentrated in three countries: Saudi Arabia, Iran and Jordan, with no primary studies identified for Comoros, Djibouti, Libya, Mauritania and Somalia. This further highlights the variation across EMR countries in terms of resources and capacities. As for study designs, there was a predominance of descriptive studies, with effectiveness/intervention studies making up less than 13% of all papers. Only two systematic reviews were identified, one focusing on quality of care in PHC in the EMR and the other focusing on weaknesses and challenges of PHC in Iran. Despite the multidimensional nature of quality, the included studies largely assessed quality of care using a single dimension. Moreover, the potential of multisectoral collaboration remains untapped in almost all countries, despite a growing realisation of its importance for reducing health inequities.56 57 These findings reflect the limited lens through which quality, patient safety and performance management are approached in the EMR.
Findings also bring to attention the status of research on quality, safety and performance management in PHC in war zones, conflict settings, protracted refugee situations or in refugees’ host communities in the EMR. Despite the magnitude of the humanitarian emergencies taking place in the EMR,58 only 32 studies addressed quality, safety and performance management in PHC in these settings. Countries of focus were Palestine (n=15), Jordan (n=7), Lebanon (n=3), Sudan (n=3), Iraq (n=2) and two or more EMR countries (n=2). None of the studies were conducted in Syria, Yemen, Somalia or Libya to investigate the effects of recent, or ongoing conflicts on the quality, safety and performance of PHC. Topics such as provider and patient safety, patient-reported outcomes and knowledge of patients were not assessed in any of those studies. The importance of examining and improving the quality of healthcare received by people in fragile settings has been recently emphasised in order to achieve UHC by 2030.59
The top five research priorities that emerged from overall ranking of all policy-makers related to: establishing national and regional quality and patient safety indicators; implementing risk and safety management approaches; promoting rational drug prescribing; enhancing equitable access to PHC; and training of clinicians in quality improvement. These likely correspond to priorities that are policy-relevant, urgently needed, feasible to implement and applicable to the local context, with expected positive impact on health. There was some fluctuation in ranking by study country which may reflect the different background and interests of key informants as well as their perceived impact in addressing these research priorities. Nonetheless, the issue of ensuring equitable access to care among vulnerable population was ranked among the top five priorities in almost all study countries. This likely reflects the protracted refugee situations or internal conflicts experienced by these countries, which have implications on access to healthcare. Previous studies have indicated that the EMR countries still lag behind others in achieving health equity60; thus addressing this question is critical given that strong pro-equity agenda is a prominent feature of PHC in the SDG era.
The proposed approach for research implementation can help promote evidence-informed health policy-making and practice by aligning research production to policy priorities and using several knowledge translation products, platforms and tools to impact policy agendas and action. This is particularly relevant in the context of the EMR where there is misalignment between actual research production and policy priorities, and inadequate knowledge uptake activities to promote the use of evidence in policies and practice.55 61 62
Strengths and limitations
A strength of this study is that it responds to the needs of policy-makers and stakeholders in the EMR. We followed the JBI guidelines and PRISMA Extension checklist for conducting and reporting scoping reviews, and a method review of the literature to build the gap maps. For the priority setting meetings, we sampled a diverse group of high-level policy-makers along with academia and non-governmental organisation (NGOs) across the study countries and used evidence-based multicriteria decision analysis to rank the priorities. Additionally, the proposed approach for research implementation spans the entire knowledge spectrum linking priority setting to research production and knowledge translation.
Some of the potential limitations of this study are discussed below. First, we acknowledge that there may be some areas of overlap in the categorisation of themes according to the conceptual framework for quality, safety and performance management in PHC. However, we attempted to minimise this through continuous inputs from all team members. Second, despite our effort to enhance comprehensiveness of the scoping review, we may still have not captured potential studies not listed on the search engines used. Also, due to resource and time constraints, we included four countries from the region in the priority setting meetings, thus the list of ranked questions may not be generalisable to all EMR context. However, care was taken to ensure the included countries reflected the diversity of the region. Moreover, the evidence and gap maps generated encompass EMR countries, and thus, could inform future priority setting exercises beyond the study countries.
Implications for research and policy
Study findings can help inform and direct future plans to generate, disseminate and use research evidence to enhance quality, safety and performance management in PHC in the EMR and beyond. By bringing the attention of researchers, funding agencies and policy-makers to the research gaps, priority questions and proposed approach for research implementation, this study could help bridge the gap between research and policy and contribute to the development of evidence-informed policies and practices in PHC. This comes at a critical time when the EMR is facing rapid demographic and epidemiological transitions, unprecedented migrations and internal displacements, escalating healthcare costs and rising expectations for high quality services. Moreover, it responds to global efforts to make research more valuable by avoiding duplication of research and reducing research waste.63
Study findings can also inform the work of the WHO Eastern Mediterranean Regional Office (WHO EMRO) who have highlighted a need to identify priority questions in the area of quality and safety in the EMR.26 WHO EMRO can provide technical support to ensure the priorities generated from this study become integrated into current and future strategic plans of ministries of health and related ministries in study countries.
An additional contribution of this study is the development of a transparent and reproducible methodology for research prioritisation, which can be adapted by other countries in the EMR and beyond.
Acknowledgments
We would like to acknowledge Ms. Aida Farha for validating the search strategy developed for the scoping review. We would also like to acknowledge Ms. Ruba Abla, Ms. Najla Daher and Ms. Rand El Ghossaini, for their support in writing and proof-reading the original report.
References
Footnotes
Handling editor Valery Ridde
Contributors FEJ, RF and LB contributed to the conceptualisation and design of the study. RF, LB and LH designed and performed the search strategy. RF, LB, LH, AA, IT and NH contributed to screening, data extraction, data analysis and development of gap maps. FEJ, RF, LB, RSH, RA, RRH and CA contributed to generation of initial list of priority questions, refinement of questions, conducting actual priority setting exercise and generation of ranked priority questions. FEJ and RF interpreted the results and developed the research implementation plan. RF wrote the first draft of the manuscript. All authors critically reviewed and approved the final version of the manuscript. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This publication is based on research funded by Ariadne Labs through Brigham and Women’s Hospital, which is the recipient of a Bill and Melinda Gates Foundation grant. The findings and conclusions contained within are those of the authors and do not necessarily reflect positions or policies of the Bill & Melinda Gates Foundation.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Institutional Review Board of the American University of Beirut.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data relevant to the study are included in the article or uploaded as supplementary information.