Article Text

Abstract
Introduction The aim of this study was to assess the effectiveness of a patient-held health record (PHR) for asylum seekers on the availability of health-related information.
Methods An explorative, cluster-randomised stepped-wedge trial with reception centres as unit of randomisation was conducted. All reception centres (n=6) in two large administrative areas in South Germany with on-site health services were included. All physicians working at these centres were invited to participate in the study. The intervention was the implementation of a PHR. The primary outcome was the prevalence of written health-related information. Secondary outcomes were the physicians’ dissatisfaction with the available written information and the prevalence of missing health-related information. All outcomes were measured at the level of patient–physician contacts by means of a standardised questionnaire, and analysed in logistic multi-level regression models.
Results We obtained data on 2308 patient–physician contacts. The presence of the PHR increased the availability of health-related information (adjusted OR (aOR), 20.3, 95% CI: 12.74 to 32.33), and tended to reduce missing essential information (aOR 0.71, 95% CI: 0.39 to 1.26) and physicians’ dissatisfaction with available information (aOR 0.5, 95% CI: 0.24 to 1.04). The availability of health-related information in the post-intervention period was higher (aOR 4.22, 95% CI: 2.64 to 6.73), missing information (aOR 0.89, 95% CI: 0.42 to 1.88) and dissatisfaction (aOR 0.43, 95% CI: 0.16 to 1.14) tended to be lower compared with the pre-intervention period.
Conclusions Healthcare planners should consider introducing PHRs in reception centres or comparable facilities. Future research should focus on the impact of PHRs on clinical outcomes and on intersectoral care.
Trial registration ISRCTN13212716. Registered 24 November 2016. Retrospectively registered. http://www.isrctn.com/ISRCTN13212716
- asylum seekers
- refugees
- migration
- continuity
- health services
- health information
- health record
- medical record
- cluster randomisation
- stepped-wedge trial
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- asylum seekers
- refugees
- migration
- continuity
- health services
- health information
- health record
- medical record
- cluster randomisation
- stepped-wedge trial
Key questions
What is already known?
Healthcare for asylum seekers is often fragmented and impeded by a high number of involved healthcare providers, frequent moves, unstandardised recording of health problems and language barriers.
These factors result in a loss of health-related information, unnecessary repeat examinations and insufficient patient follow-up.
Strategies to improve continuity of care for displaced populations who are often accommodated in reception centres are urgently needed.
What are the new findings?
This first cluster-randomised stepped-wedge study provides evidence for a positive impact of a patient-held health record (PHR) for asylum seekers on continuity of care.
The PHR substantially improved the prevalence of health-related information, and tended to reduce missing essential information and physicians’ dissatisfaction with the available information.
What do the new findings imply?
PHRs are an appropriate tool to improve the availability of health-related information of asylum seekers.
Healthcare planners should consider using PHR in reception centres or comparable facilities.
Introduction
The number of forcibly displaced persons has been increasing in the recent years and reached a record high of 68.5 million worldwide by the end of 2017.1 Providing appropriate healthcare for displaced population groups remains one of the largest challenges for the host countries and the international community.
In Germany, about one million refugees have been recognised by the end of 2017.2 People seeking asylum in Germany are initially accommodated in the so-called ‘first reception centres’ (Landeserstaufnahmestellen) organised by the federal states and later on transferred to peripheral state-mandated reception centres or collective accommodations organised by the respective communities. The healthcare provided in the first reception centres does not follow any national guideline and is very heterogeneous, for example, regarding the type of services provided, the equipment, the number of health personnel or the procedure for referrals. Also the way of documenting patient data and the course of treatment is diverse: While in some reception centres, electronic documentation systems are established (which are usually not compatible with each other so that automatic data transfer is impossible in case a patient is transferred to another centre), other reception centres rely on paper-based documentation. There is no uniform procedure for handing out the medical documentation to the asylum seekers—frequently they do not receive any written information about their treatment. Yet, a screening for tuberculosis is conducted in all 16 German federal states.3 Some reception centres do not have on-site healthcare clinics but refer all asylum seekers in need for medical care to nearby reception centres, hospitals or practices. After transfer to the communities, asylum seekers receive healthcare from the regular local primary and secondary care providers, but services are restricted to healthcare for acute and painful conditions or essential needs.4
The average time an asylum seekers spends in the first reception centre before being transferred to a community ranges from a few days up to the entire length of the asylum process. The average duration of an asylum procedure is about 12 months, with substantial variation between countries of origin (ranging from 7.8 months for Syrians to 17.2 months for applicants from the Democratic Republic of Kongo).5
In many cases, asylum seekers are subject to multiple transfers to various centres and accommodations and frequently these transfers are announced only one or a few days ahead. This often leads to disrupted care as health professionals are usually not informed about transfers.
Besides such ‘within-country flows’, a considerable number of asylum seekers apply for asylum in several countries leading to ‘cross-border flows’.
The high number of healthcare providers involved in the treatment, the frequent, spontaneous moves, the unstandardised documentation and language barriers make it extremely difficult to guarantee continuity of care. This may cause a loss of information resulting in unnecessarily repeated examinations and insufficient follow-up of the patient.6 7
A recent study concluded that under these circumstances a patient-held health record (PHR) for asylum seekers can be a viable solution to improve the sharing of medical information.6 Several systematic reviews examine the use of PHRs in routine care settings, for example, in cancer care,8 obstetrics,9 paediatrics10 11 or chronic disease management.12 While most of the reviews show no or modest effects of PHRs on clinical outcomes, patients usually find them very helpful and healthcare professionals see some benefit. To our knowledge so far, no studies evaluating PHRs for asylum seekers have been conducted, so the effect and usefulness of a PHR in such a special setting remains unclear.
In 2016, a PHR for asylum seekers was piloted in one first reception centre in Heidelberg, South Germany and later on implemented by the local state authorities in the reception centres in two other areas (Mannheim and Karlsruhe) in Baden-Württemberg, the third largest federal state in Germany. A stepped-wedge cluster-randomised trial accompanied by a comprehensive process evaluation was performed to evaluate the usefulness and effectiveness of the PHR.
The criteria when a stepped-wedge design might be superior to a parallel design are well described13 and all apply to this study: First, stakeholders decided to implement the PHR in the reception centres because there was an urgent need to improve the documentation of medical data, that is, it was desired that all clusters should receive the intervention as soon as possible. Second, the pilot phase had provided evidence of the preliminary effectiveness of the PHR and third, a sequential rollout seemed to be more feasible than a rollout en bloc because the implementation of the PHR was a complex process comprising the elaboration of individual implementation concepts and instructions for the health personnel in the reception centres and the surrounding practices and clinics.
While a qualitative study examined barriers and facilitators for the implementation of the PHR,14 this study focuses on the quantitative effects of the PHR. The hypothesis was that a PHR for asylum seekers in reception centres improves the transfer of health-related information between providers and healthcare sectors and thereby continuity of care.15
Methods
The study was approved by the ethics committee of the University of Heidelberg (S-438/2016) and retrospectively registered in an acknowledged trial registry (ISRCTN13212716), as severe time constraints did not allow for prospective registration. The reporting follows the CONSORT statement for cluster-randomised trials and the modifications suggested for stepped-wedge designs.16
Design
We performed an explorative, stepped-wedge cluster-randomised trial with reception centres as unit of randomisation. Randomisation referred to the sequence of introducing the intervention in the various centres. To be able to examine the effect of the PHR on intersectoral information transfer, it was planned to collect data additionally in the so-called ‘sentinel practices’ (definition see eligibility criteria) in the surroundings of the respective reception centres.
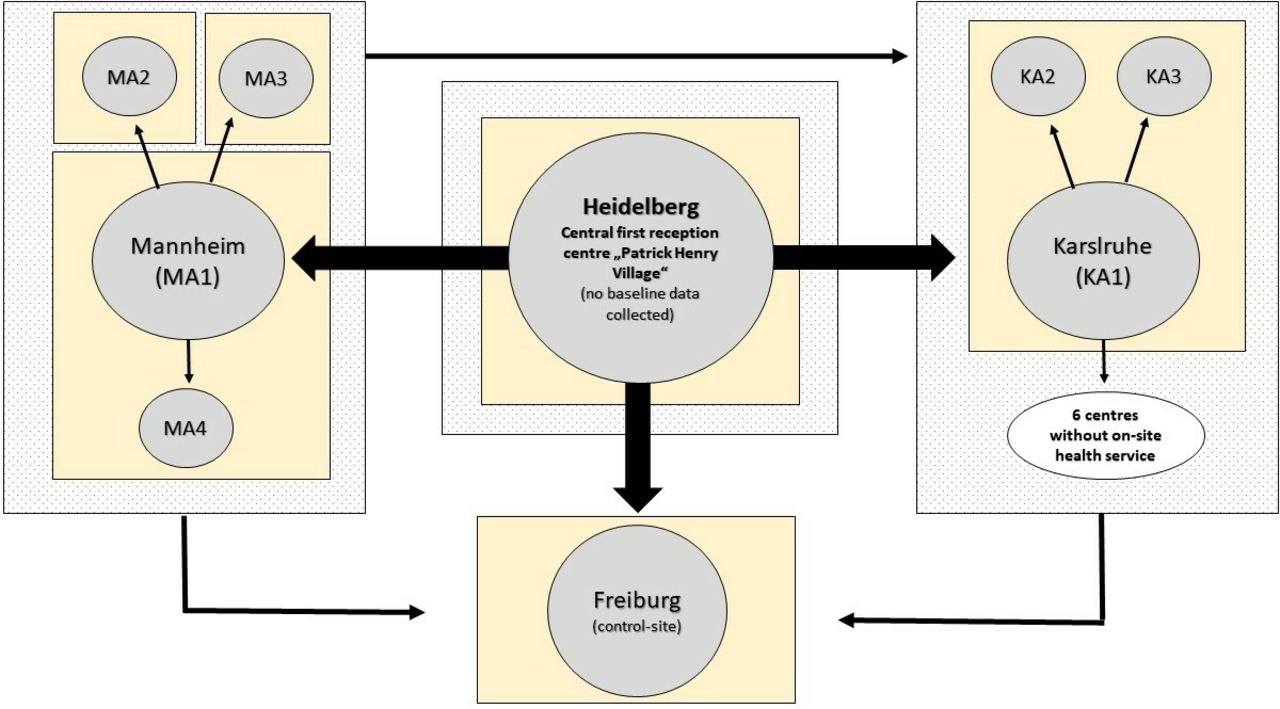
Figure 1 shows the clustering of and the patient flow between the reception centres in the study region and figure 2 shows the randomisation of the clusters and the data collection. In total, there were 15 reception centres of which eight met the inclusion criteria. The assignment of the centres described in figure 1 resulted in six clusters available for randomisation of which five received the intervention.
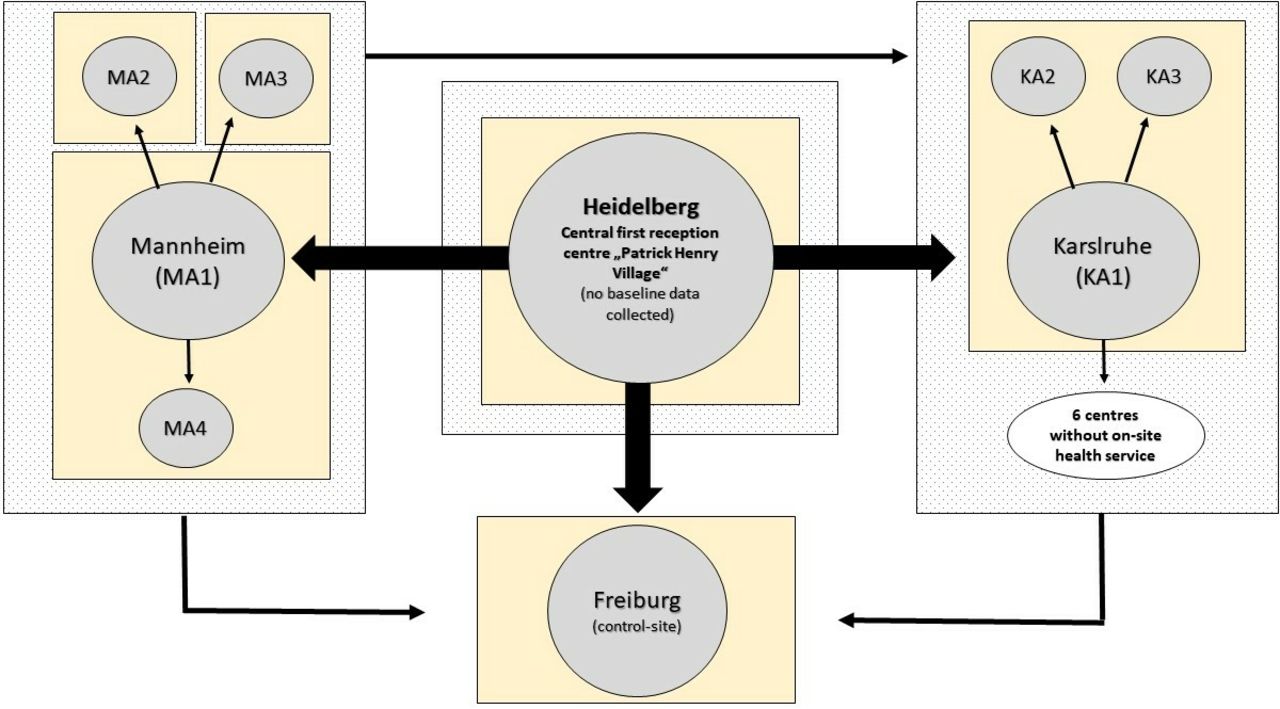
Clustering of and patient flow between the reception centres in the study areas. The PHR was implemented in all reception centres (Heidelberg, Mannheim, Karlsruhe) of one large administrative area (spotted boxes) in the federal state of Baden-Württemberg with on-site healthcare service (grey circles). The reception centre in Heidelberg had already implemented the PHR during the pilot phase, that is, no baseline data could be collected there. Freiburg did not belong to the administrative area, that is, no funds for implementing the PHR there were provided. Therefore, Freiburg served as a control site only. The centres in Karlsruhe were treated as one cluster since asylum seekers were frequently transferred between the three centres which did not allow strict separation of centres with and without PHR. In Mannheim, a very small reception centre hosting only few asylum seekers and a larger centre were treated as one cluster. All asylum seekers allocated to the federal state of Baden-Württemberg are registered in the central first reception centre in Heidelberg. After registration, they may be transferred to one or multiple other centres as indicated by the black arrows. For the evaluation study, the reception centres were bundled in six clusters (yellow boxes). PHR, patient-held health record.
{kind=link}
{kind=link}
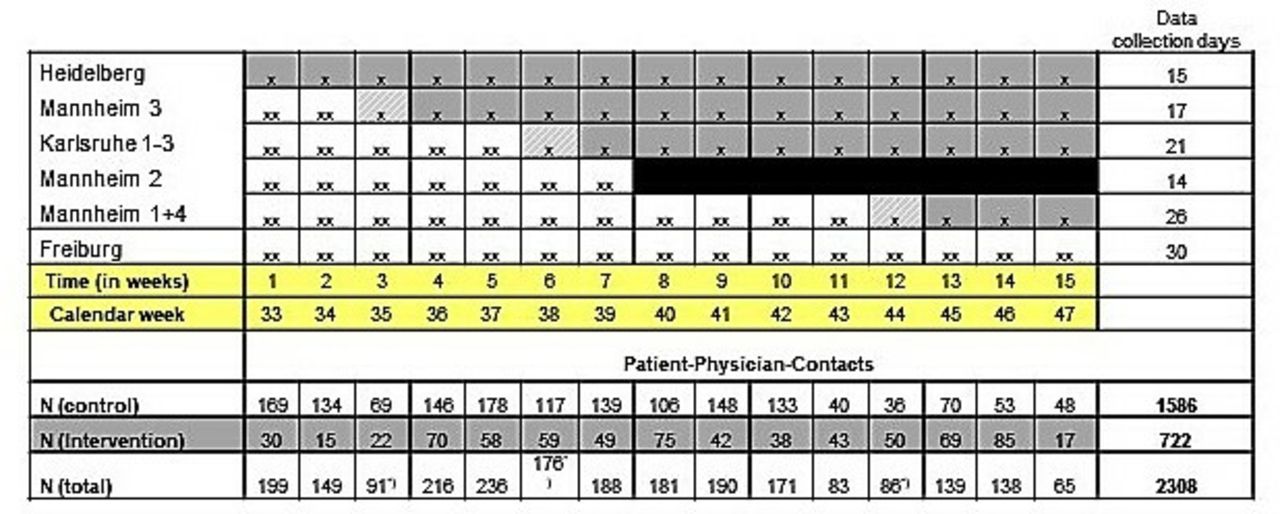
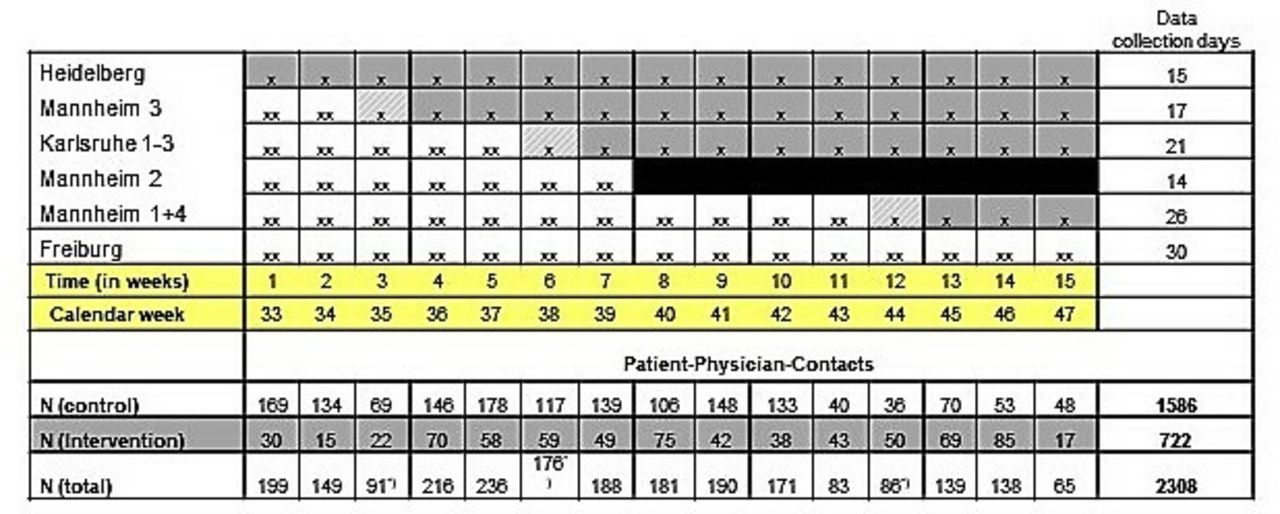
Randomisation and data collection in the clusters. Grey areas with x indicate the post-intervention data collection period (one data collection day per week), white areas with xx indicate the baseline data collection period (two data collection days per week to generate sufficiently high number of controls). The first week after implementation of the PHR was regarded as ‘transition period’ (marked with *) meaning that data were collected but not included into the analysis to allow the reception centres to establish routines for the use of the PHR and the study procedures. The reception centre Mannheim 2 was closed by the state authorities after 8 weeks so that no more data could be collected (black area). N = number of patient–physician contacts. PHR = patient-held health record.
The PHR was introduced in 3-week intervals in a new, randomly allocated reception centre so that after a time period of 15 weeks all reception centres (except the control site) had received the intervention.
The data for the primary and secondary outcomes were collected on the level of patient–physician contacts by means of a questionnaire to be completed by the physician on duty on specific dates of the week determined by a random procedure. An open study cohort was used, that is, patient data were collected anonymously during each patient–physician contact and it was not clear whether the respective patient had already participated in the baseline data collection or not. Data collected during patient–physician contacts could be linked to the physician by means of a pseudonym, and to the reception centre by means of a code for each centre.
Due to the stepped-wedge design, the number of follow-ups in the post-intervention period differed between reception centres, ranging from 12 weeks (reception centre in which the PHR was first introduced) to 3 weeks (last reception centre in which the PHR was introduced).
In the sentinel practices, all patient contacts with asylum seekers were planned to be documented.
Participants
Eligibility criteria and recruitment of study sites
The PHR was implemented in all reception centres in a large administrative area in Baden-Württemberg with an on-site healthcare service. Sentinel practices were defined as any healthcare institution (eg, emergency departments, general practices or specialist practices) to which asylum seekers are frequently referred to by physicians working in the reception centres and with at least one patient contact with an asylum seeker per week. They were identified based on the information provided by the health staff working in the reception centres.
Eligibility criteria and recruitment of patients
Since the intervention was a ‘real-life intervention’ delivered on an organisational level of healthcare facilities and not an individual study procedure, patients were not actively included into or recruited for the study. Details are explained in the section ‘implementation of the intervention’.
Eligibility criteria and recruitment of physicians
All physicians working in the reception centres who were on duty on the data collection days were eligible to participate in the study. Based on the duty rosters of the reception centres, a list of all eligible physicians was created. All were contacted by phone or email, informed about the content and course of the study personally and asked to give their written informed consent. Sentinel practices outside the reception centres were contacted by means of written invitation letters and telephone follow-ups.
Interventions
The intervention consisted of the introduction and routine use of a PHR for asylum seekers in reception centres. Once the PHR was introduced, it was used continuously in the respective healthcare setting as follows.
Intervention development and piloting
The PHR was developed in October 2015 by the Department of General Practice and Health Services Research at the University Hospital Heidelberg, in cooperation with healthcare providers in the state’s central reception and registration centre (Patrick Henry Village). Pre-existing documentation forms of the University Hospital Heidelberg and materials developed by a publisher of medical pictograms17 and by a local network on medication safety18 were screened and partly used in modified forms for the design of the PHR. Physicians working in the Patrick Henry Village were asked to provide feedback on form and content of the PHR.
The final first version of the PHR was a small booklet (148×210 mm) with 15 pages comprising (a) patient information about the booklet in 10 languages (Albanian, Arabic, Dari/Farsi, German, French, Romanian, Russian, Serbian, Tigrinya and Urdu), (b) information for doctors in German on how to use the booklet, (c) a small pocket to insert documents, (d) a table for chronic diseases, (e) a medication schedule for long-term medication, (f) a table for continuous documentation of consultations, (g) a table for test results and (h) a table for upcoming medical appointments. The same PHR was used for all patients, there were no different versions, for example, for different ages, genders, languages or medical conditions.
The first version of the PHR was introduced as a pilot in February 2016 in one reception centre (Patrick Henry Village).
Patient and public involvement
Based on the feedback from the healthcare providers using the PHR, adaptions in format and content were made. However, we did not involve patients or the public into the development of the PHR.
Implementation of the intervention
Due to the positive feedback of practitioners during the pilot phase, the local state authorities decided to cover the costs of implementation and provision of the PHR in all reception centres with on-site health services in one large administrative area in the federal state of Baden-Wuerttemberg. Thus, the provision of the PHR was not a study procedure but a real-life intervention which would have taken place even if the study had not been conducted. Local state authorities and healthcare providers in reception centres were responsible for both implementation and continuous use of the PHR. An announcement was published in national and local newspapers and information letters were sent to all sentinel practices in the surrounding areas of the reception centres to inform all medical staff potentially involved in provision of medical services to asylum seekers about the use and purpose of the PHR. Incentives for the use of the PHR were not provided.
Control
In the control period (before introducing the PHR) all reception centres continued their habitual procedures for recording health-related information of asylum seekers using either paper-based or electronic medical records. Due to the patient flow between centres depicted in figure 1 it was possible and unavoidable that the health staff got in contact with the PHR already in the control period.
Outcomes and other measures
The primary outcome was the prevalence of health-related information (eg, about previous diseases and examinations, medication, vaccination status) at level of respective physician–patient contacts.
Secondary outcomes were the prevalence of ‘missing essential health-related information’ (according to the judgement of the treating physician) and the physician’s dissatisfaction with the prevalent health-related information during the respective physician–patient contact.
Beside the outcome measures, sociodemographic data of patients and physicians as well as process data on the course of the patient–physician contact were collected.
Data collection
The primary and secondary outcomes were measured by means of a self-developed, pre-tested one-page questionnaire in German language (an English translation is provided by online supplementary file 1). It contained—beside the pseudonym of the treating physician—the following physician-reported, anonymised patient and process data:
Supplemental material
Year of birth
Nationality
Number of severe diseases
General condition (5-point Likert scale)
Intake of long-term medication (yes/no)
Whether and how language mediation was necessary (nominal scale, multiple answers possible)
To which extent, it was possible to get the necessary information during the consultation (5-point Likert scale)
Whether the patient had a PHR with him/her (yes/no)
Whether any written information about the patient’s history was available (yes/no) (primary outcome)
The type of written information (nominal scale, multiple answers possible),
Whether relevant information was lacking (yes/no) (secondary outcome)
How satisfied the physician was with the available medical information during this encounter (5-point Likert scale collapsed into a binary variable consisting of dissatisfied ‘very bad/bad’ and satisfied ‘very good/good/moderate’) (secondary outcome)
How helpful the PHR was (10-point scale).
The physicians completed one questionnaire for each patient–physician contact on the data collection days (about 1–2 min per questionnaire). Additionally, they provided once-only sociodemographic specifications about themselves. Details of the data collection are described in the trial design section.
Sample size and sample size justification
Since no data were available on the expectable effects of the PHR and since the number of clusters was already determined (local state authorities decided to implement the PHR in all reception centres providing medical services in a defined region) and since no comparable previous studies were available to estimate the effect of the intervention no statistical sample size calculation was performed. Yet, based on the experiences of the healthcare providers and specifications of the local state authorities, the number of expected patient–physician contacts were calculated before the trial started. As the figure in online supplementary file 2 shows, it was assumed that in total 3880 relevant patient–physician contacts would take place during the entire data collection period in all clusters and sentinel practices. Due to the heterogeneous care settings, the participation rate of physicians and the completeness of documentation could not be reliably estimated in advance.
Supplemental material
Every 3 weeks, the intervention was introduced in a new cluster. This interval was chosen to ensure sufficient time between the starting points of the individual sites while limiting overall trial duration. This was relevant, as continuous data collection took place on all participating sites independently of the starting point of the intervention.
Randomisation and allocation concealment
Randomisation was performed by a study nurse at the Department of General Practice and Health Services Research who was not involved in study design or data collection. Centres were coded by the research team. The study nurse received the centre codes, concealed them in closed envelopes, and drew one envelope every 3 weeks (simple random sampling without replacement).
Allocation of clusters to the intervention and the randomly determined data-collection days remained concealed towards the authorities in charge of implementing the PHR and the physicians.
Blinding
Due to the nature of the intervention and the trial design (all clusters received the intervention), blinding of the medical staff was not possible. However, patients were not aware of the evaluation study because the PHR was implemented as part of the routine processes for all asylum seekers and because patients were not involved in the data collection.
Statistical analysis
Means and proportions stratified by time before versus after introduction of the PHR were calculated for interval-scaled and categorical data, respectively. We analysed the effect on primary and secondary outcomes following two analytical strategies with respect to exposure to the intervention. Strategy 1 used the presence of the PHR (yes/no) in a patient–physician contact as independent variable, and strategy 2 used the time before versus after (coded 0/1) the introduction of the PHR in each cluster as independent variable. For each strategy, we analysed the effect on primary and secondary outcomes in single and multiple logistic regression models by calculating adjusted ORs (aORs) and 95% CIs. We fitted two-level logistic regression models with patient–physician contacts (level 1) nested in physicians (level 2), applying generalised linear mixed models by maximum likelihood (adaptive Gauss-Hermite Quadrature) functions. Three-level models were tested, but showed lower model fit as no significant clustering was observed at level of the reception centres.
A total of six multivariate models were built, and each model was mutually adjusted for the following covariables hypothesised to function as confounder of the association between independent variables and outcome: physicians’ age and sex, patients’ age and sex, presence of chronic morbidity, presence of language barriers, and presence of health-related information in electronic health records. We excluded three patient–physician contacts from the analysis due to implausible year of birth of treated patients (born before 1920), and 55 contacts which occurred in the transition phase (figure 2). Explorative subgroup analyses were performed for strata of patients with/without chronic morbidity, and for those with/without long-term prescriptions. Missing data were treated as missing at random and a complete case analysis was performed without imputing data.
Results
Participant flow and recruitment
The data collection started on 23 August 2016 and ended on 02 December 2016. Figure 2 shows the number of patients–physician contacts evaluated in each cluster before and after introduction of the PHR. In total, 55 physicians participated in the data collection and documented 2308 patient–physician contacts: 1586 before and 722 after introduction of the PHR. Due to a lack of routine documentation, we do not know the number of the actual patient–physician-contacts and are thus unable to determine the participation-rate. No physician actively withdraw consent for participation.
Characteristics of the sample and descriptive data
Table 1 shows the characteristics of the sample. The asylum seekers consulting the on-site clinics in the first reception centres were on average 29 years old (range: 1–95 years). About one-third of the patients (30.8%, n=630) were women. The most frequently specified countries of origin were Gambia (24.8%, n=474), Nigeria (12.9%, n=247), Eritrea (9.0%, n=173), Cameroon (6.8%, n=130), Macedonia (5.3%, n=101), Serbia (5.3%, n=101), Afghanistan (4.5%, n=87) and Albania (4.5%, n=86). According to the judgements of the treating physician, about 70% (n=1576) were in a good or very good general condition. About one-quarter of the asylum seekers (22.6%, n=630) suffered from one or more known severe diseases and 17% (n=279) took long-term medication.
Patient characteristics and descriptive outcome data
In the intervention period, the PHR was present during 71% (n=501) of the patient–physician contacts. The fact that the PHR was also present in 6.8% (n=106) of the patient–physician contacts during the control period is a result of the patient flows depicted by figure 1. In the majority of patient–physician contacts (63.1%, n=1489), physicians and patients were able to communicate in a common language (usually English or French). Translators—usually laypersons—were used in 28.8% (n=678) of the contacts. If written medical information was available—which was the case in 30% (n=648) of the patient–physician contacts—it referred to previously known diagnoses or diseases (63.1%, n=409), previous examinations (51.4%, n=333), previous treatments (50.0%, n=298), medication (39.8%, n=258) or other information (5.7%, n=37).
In 40% (n=917) of the consultations physicians reported inability to obtain the necessary medical information during the conversation and in 81% (n=1630) of the consultations physicians reported that important written medical information was missing. The available health-related information was judged as ‘bad’ or ‘very bad’ in 12% (n=258) of the patient contacts.
Table 2 shows the characteristics of the participating physicians and of the clusters. The number of physicians per cluster ranged from 1 to 26. The average age was 53 years (range: 32–77 years). The perceived helpfulness of the PHR (assessed by a 10-point score) ranged on average from 4.9 to 8.2 points and varied between clusters.
Characteristics of physicians and clusters
Effects of the intervention on primary and secondary outcomes
Comparing patient–physician contacts with and without PHR, we found that the adjusted odds that written health-related information was present during the respective patient–physician contact was 20 times higher (OR 20.3, 95% CI: 12.74 to 32.33) if a patient carried a PHR (table 3). The adjusted odds that important information was missing decreased by a factor of 0.71 (aOR 0.71, 95% CI: 0.39 to 1.26) with a PHR compared with patient–physician contacts in which no PHR was carried by patients. The dissatisfaction with the available health-related information was lower if a PHR was present (aOR 0.5, 95% CI: 0.24 to 1.04), adjusted for all covariables (table 3).
Primary and secondary outcomes comparing contacts with and contacts without PHR
Comparing patient–physician contacts before and after introduction of the PHR, we found that the adjusted odds of written health-related information being present during the respective patient–physician contact after introduction of the PHR was four times the adjusted odds before introduction of the PHR (aOR 4.22, 95% CI: 2.64 to 6.73) (table 4). After introduction of the PHR the adjusted odds that important information was missing was lower compared with the period before the intervention (aOR 0.89, 95% CI: 0.42 to 1.88). The dissatisfaction with the available health-related information was reduced after introduction of the PHR (aOR 0.43, 95% CI: 0.16 to 1.14) (table 4).
Primary and secondary outcomes comparing contacts in the period before versus after introduction of the PHR
We did not analyse data from sentinel practices as the participation rate was extremely low.
Subgroup analysis
We found a positive effect of the PHR on the prevalence of written health-related information in patients without long-term medication (aOR 29.74; 95% CI: 15.49 to 57.08), which was stronger than the effect observed in those with long-term medication (adjusted OR 10.11, 95% CI: 3.82 to 26.71). Similarly, the effect was stronger in patients without severe conditions (aOR 28.69; 95% CI: 16.30 to 50.46) than in patients with severe diseases (aOR 9.29; 95% CI: 4.24 to 20.32).
Harms
No critical events were observed or reported to us. Possible unintended negative effects of the PHR (eg, stigmatisation of patients with certain conditions or infringement of patient autonomy due to local manners of using the PHR) are described in a qualitative evaluation study.14
Discussion
This study showed that a PHR for asylum seekers implemented in reception centres has the potential to substantially improve the transfer of medical information between different healthcare providers within and between reception centres. If a patient had the PHR with him or her at the doctor’s appointment, it was 20 times more likely that health-related information was available, even if the PHR was not yet introduced at the centre adjusted for relevant individual-level and institutional-level factors. We found consistent trends towards lower prevalence of missing essential information, and lower odds for dissatisfaction of physicians with health-related information during patient–physician contacts when the PHR was present. Consistently, the chance that written health-related information was available during the patient–physician encounter was in average four times higher after implementation of the PHR than in the period before, adjusted for patient-, physician- and institutional-level factors. This finding indicates that the process of implementing a PHR has an intervention effect at population-level by itself, even if the PHR may not be used consistently for all patients afterwards. The adjusted odds that essential information was missing and that physicians are dissatisfied with health-related information was in average lower after intervention compared with the period before, although these were trends and not statistically significant.
The finding that the effect of the PHR on the prevalence of written health-related information was stronger in patients without long-term medication and without severe chronic conditions deserves attention. One possible explanation is that patients with complex medication regimes and multiple chronic conditions frequently have a long medical history and usually have to archive a high number of medical reports so that it is more likely that they carry information with them even without a PHR in place compared with patients with acute and non-complex conditions. Furthermore, the PHR has only capacity for a few documents and short notes. Although the PHR effectively improved the availability of information among patients with long-term medication compared with contacts without PHR among these patients, its capacity to carry all required health-related information of complex patients is certainly limited.
The strong effects shown in this trial have to be interpreted in the light of the findings of an accompanying qualitative study which examined barriers and facilitators for the implementation of the PHR, including detailed process evaluation.14 The study showed that how the PHR was implemented, used and perceived, differed between reception centres, healthcare providers and patients. For example, in reception centres in which an electronic medical records system was used, the PHR was regarded as less helpful to improve availability of information during patient encounters. While the relevance of using the PHR for physicians after transfer was acknowledged, concerns existed due to the additional work and duplicate documentation. Limited routines for informing all healthcare providers and especially patients about the existence and purpose of the PHR were seen as another major barrier. Furthermore, individual behaviours limited the full potential of the PHR, for example if the documentation was incomplete or illegible or if patients did not actively show their PHR to the healthcare providers.
Considering the quantitative findings presented here and the qualitative insights of the PHR evaluation,14 we recommend to consider introducing PHRs for asylum seekers in reception centres or comparable facilities to improve the documentation and transfer of health-related information, especially if no electronic medical records system is established or if exchange of health-related information is not possible despite electronic systems (eg, due to data protection issues or system incompatibility). Authorities in charge of reception centres should not only cover the costs for PHRs but also provide funds for comprehensive implementation activities (eg, trainings, campaigns, elaboration of individual implementation action plans) to make sure that the entire target population is informed and convinced of the purpose of the PHR and that the prerequisites for its correct used are provided. While we evaluated the implementation of a locally developed PHR, the findings may be transferable to other PHRs developed by other agencies, for example, PHR of the International Organisation for Migration.19–21 However, as each of the PHRs is designed differently, their practicability and capacity to carry health-related information of patients during contacts and repeat-contacts may differ.
Our study results need to be interpreted taking into account important strengths and limitations. The study examined an organisational level ‘real-life intervention’ conducted in multiple reception centres with different prerequisites and documented a high number of patient–physician contacts using a rigorous cluster-randomised study design. Therefore, we are confident that the effects shown by the study are reproducible in other settings under real-life conditions.
However, there were some deviations from the study protocol: The participation rate in the sentinel practices was extremely low so that it was not possible to examine the effect of the PHR on intersectoral care outside reception centres as intended. Participation of physicians was voluntary but we were unable to determine the participation rate as the total number of physicians working in the reception centres was unknown. Therefore, a selection bias in favour of the intervention cannot be excluded.
Furthermore, although the instrument was pre-tested, it was not formally validated and used in previous studies, which is also due to the fact that, as far as we are aware, this was the first study of its kind assessing these outcomes.
The study focused on the prevalence of written information and of missing information while the impact of the PHR on clinical outcomes such as avoidable repeat examinations, hospitalisations or treatment errors, was not assessed due to lack of data on these outcomes and weaknesses of the German health information system to obtain such information for asylum seekers.22
We chose to use dichotomous variables for the outcome analysis (written medical information available yes/no, important medical information lacking yes/no) and did not take into account the type of information. Although this is certainly of clinical relevance, the subgroup of patient–physician contacts for which the type of written medical information was documented was too small for such an analysis.
Patients were not involved into the development and design of the PHR. Considering the patient perspective may improve the comprehensibility and usability of the PHR.
Conclusions
PHRs for asylum seekers implemented in reception centres proved to be an effective tool to improve the availability of written health-related information. The PHR tended to reduce missing essential information and improve satisfaction with health-related information needed to make medical judgements. Due to the rigorous and innovative design of the study, we are confident that the effects shown in this trial could be reproducible in other settings and recommend considering the use of PHRs for asylum seekers in reception centres or comparable facilities, especially if no electronic medical records system is used. Funds for accompanying implementation activities should be calculated. Future research should focus on the effect of PHR on intersectoral care and on clinical or patient-reported outcomes as well as on further assessments of instruments to measure health-related information transfer.
Acknowledgments
The authors thank the participating physicians, all supporting health personell, the regional administrative council Karlsruhe (Regierungspräsidium Karlsruhe) and Freiburg (Regierungspräsidium Freiburg) as well as the University Hospital Freiburg for supporting this study. We acknowledge the contribution of Sandra Gewalt in collecting the data. The authors thank Lorenz Uhlmann for statistical support.
Footnotes
Handling editor Dr Eduardo Gómez
Contributors Author Contributions: Conceived the study: KB. Study design: KB, SN, CS. Data collection: CS, SZ, RJ, KW. Development of methods and measures: SN, KB, CS. Data analysis: SP, KB. Interpretation: SP, KB, CS. Writing of first and final version of the manuscript: CS, KB. Revision for important intellectual content: CS, SN, SP, RJ, SZ, KW, KB. All authors approved the final version for publication.
Funding The study was funded by the Federal Ministry of Education and Research (BMBF) within the scope of the RESPOND project ('Improving Regional Health System Responses to the challenge of forced migration through tailored interventions for asylum seekers and refugees', grant number: FKZ 01GY1611). The funder did not have any role in the study design or in the collection, analysis, interpretation and publication of data.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study protocol was approved by the ethical committee of the Medical Faculty of the University of Heidelberg (Ethical approval nr: S-438/2016).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement De-identified participant data are available from the last author (Kayvan Bozorgmehr, kayvan.bozorgmehr@med.uni-heidelberg.de, ORCID
0000-0002-1411-1209) upon reasonable request.