Article Text

Abstract
Introduction The adverse physical consequences of female genital mutilation/cutting (FGM/C) have been thoroughly investigated and documented. Yet, we know little about the adverse mental health consequences of the practice. To fill this research gap, we systematically reviewed studies that assessed any adverse mental health consequences related to FGM/C.
Methods We searched four databases from inception to 21 December 2018. We then reviewed all titles and abstracts for relevant studies. We used the National Institutes of Health quality assessment tool to appraise the quality of each study and the Newcastle-Ottawa Scale to rate the risk of bias within studies.
Results We included 16 studies in this review; only six studies examined the association between FGM/C and adverse mental health outcomes as the sole research question. Among the included studies, 10 were conducted at the participants’ country of origin. The sample size of the populations studied ranged from 3 to 4800 participants. Only one study received a rating of ‘good’ methodological quality.
Fourteen of the 16 studies reported an association between FGM/C and at least adverse mental health outcome. These included eight studies that reported a higher burden of adverse mental health outcomes among women who underwent FGM compared with women who did not undergo FGM/C. Four studies reported a correlation between the severity of FGM/C and the severity of adverse mental health outcomes.
Conclusion This systematic review documents an association between FGM/C and adverse mental health outcomes. Importantly, our review demonstrates the need for more rigorous research on the topic.
- female genital mutilation/cutting
- FGM/C
- depression
- PTSD
- anxiety
- mental health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
There are more than 200 million women and girls who have undergone female genital mutilation/cutting (FGM/C), living in 30 countries around the globe. Further, about 3 million girls remain at risk of being subjected to FGM/C annually.
There has been an increased interest in studying the adverse health outcomes associated with FGM/C over the past few decades. The adverse physical consequences of FGM/C have been thoroughly investigated and documented. We know, however, very little about the adverse mental health consequence of the practice.
Despite poor mental health being cited as a consequence of the practice in most reports on FGM/C, data documenting the prevalence and severity of such consequences are sparse.
What are the new findings?
The quality of the studies assessed is generally weak.
Our systematic review documents an association between FGM/C (especially among severe cases of FGM/C) and adverse mental health outcomes.
What do the new findings imply?
Future work should create more rigorous evidence, particularly on the correlation between FGM/C type and severity of adverse mental health outcomes.
Introduction
The total number of women and girls who have undergone female genital mutilation/cutting (FGM/C) is unknown. However, the United Nations International Children’s Emergency Fund estimates that there are currently more than 200 million women and girls who have undergone FGM/C, living in 30 countries around the globe.1 Moreover, while the overall rate of the practice is declining, about 3 million girls remain at risk of being subjected to FGM/C annually.2 3 The practice is most prevalent in Eastern, Northeastern, Western regions of Africa, a number of countries in the Middle east and Asia, and asylum seekers and migrant communities from these countries—mainly to high-income countries.4 5
FGM/C refers to any practice that involves deliberately cutting, injuring or changing the external female genitalia. As such, the FGM/C ranges from ritual superficial nicks to the complete removal of the external genitalia. FGM/C is often performed for cultural, religious or other non-medical reasons; often on girls between the ages of 4 and 10.6 7 WHO identifies four types of FGM/C based on the procedure and severity; type III being the most severe.8 There is a near global consensus for the need to protect girls from undergoing FGM/C, evidenced by the fact that FGM/C is illegal in most countries.3 9 Moreover, the practice is considered a violation of the international human rights laws.5 A number of international agencies and government have recently been advocating for investing in the provision of adequate care to address the health-related consequences of FGM/C.5
Over the past few decades, there has been an increased interest in studying the adverse health outcomes associated with FGM/C. The adverse physical consequences of FGM/C have been thoroughly investigated and documented.10–13 We know, however, very little about the adverse mental health consequence of the practice. Despite poor mental health plausibly being a potential consequence of FGM/C, data accurately documenting such outcomes are sparse. Prior efforts to examine the state of the evidence on adverse mental health outcomes were often non-systematic in their approach or only reported mental health disorders in conjunction with sexual health-related outcomes of women who underwent FGM/C.14–16 To our knowledge, to date, there has been no systematic effort to synthesise the evidence that examines the adverse mental health outcomes associated with FGM/C in the public health or medical literature.
To fill this research gap, we systematically reviewed studies that assessed any adverse mental health consequences related to FGM/C. This review aimed to answer the question: what are the psychological disorders associated with undergoing FGM/C?
Methods
Search strategy
We conducted a search across the following bibliographic databases: PubMed,17 Embase,18 Web of Science19 and PsycINFO20 from inception to 21 December 2018. We present the detailed search strategies in online supplementary file 1. Overall, we combined various synonyms for FGM/C with terms focusing on mental health outcomes including various synonyms for mental health, depression, anxiety and post-traumatic stress disorder (PTSD). To maximise the number of studies identified, we applied no filters (except for a filter limiting the sex of participants to female in PsycINFO database). We also conducted a manual search of the references of included studies from the database search and prior reviews on the FGM/C to account for any records we might have missed.
Supplemental material
Study identification and abstraction
Following deduplication using the reference management software Mendeley, we screened the titles and abstracts of identified records to decide whether we should appraise the full paper using the systematic reviews web app Rayyan QCRI. We then screened full texts to determine whether to include or exclude articles. We excluded articles if the study was qualitative in nature, did not report psychological outcome(s), or if the full text was not written in English.
We abstracted included studies into an electronic form (Microsoft Excel). In the abstraction form, we summarised the research question(s), study population and sample size, psychological outcomes investigated, tools used for psychological assessment and study results. We present a flow chart, guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, describing the study selection process and number of articles retrieved, included and excluded in figure 1.

Flow chart describing the study selection process and number of articles retrieved, included and excluded.
Study quality assessment and risk of bias
No study was excluded from this review on the basis of methodological quality. We did, however, use the US Department of Health and Human Services, National Institutes of Health quality assessment tool for observational cohort and cross-sectional studies to appraise and report on the quality of each study.21 The answers to the tool measures were ‘yes’, ‘no’, ‘not mentioned’ or ‘not relevant’. We then rated the studies as of ‘poor’, ‘fair’ or ‘good’ methodological quality.
Guided by the Newcastle-Ottawa Scale for risk assessment of non-randomised trials, we then assessed the risk of bias for each of the included studies. We assessed each study on risk of bias in participant selection (representativeness, size and non-respondents to study sample), comparability (reporting on different exposure groups) and exposure/outcome relationship measurement (quality of outcome assessment methods and appropriateness of statistical methods used for analysis).22 23 For each study, we then rated levels of risk as ‘low level of risk’, ‘high level of risk’ and ‘unclear risk’. The last category indicates that the information needed for adequate assessment was inconclusive or unavailable.
Patient and public Involvement
Patients were not involved in conducting this review.
Results
We describe the research questions, study population and sample size, mental health outcomes investigated, tools used for psychological assessment, key results and methodological quality of the 16 studies included in this review in detail in table 1.
Summary of key components of the 16 reviewed studies
Research questions
Of the 16 studies we included, six focused solely on the adverse mental outcomes of FGM/C.7 24–28 The other 10 studies examined a variety of FGM/C-related health measures, including adverse mental health outcomes.29–38
Study population and sample size
Studies varied in both characteristics of populations studied and sample size. While a number of studies restricted their populations to a specific ethnic group or age category, others included a wide range of demographic characteristics. Ten studies were conducted at the participants’ country of origin: Egypt, Ethiopia, Iran, Iraq, Israel, Kuwait and Senegal7 24–27 30–32 34 35 and six studies targeted migrant women in Greece, the Netherlands, Spain and the USA.28 29 33 36–38 Seven studies examined potential adverse mental health outcomes spanning adolescence and adulthood,7 27 30–32 34 38 six studies restricted their populations to adults,25 28 29 33 36 37 two studies to adolescents24 26 and one study35 did not list participants’ age range. While the majority of studies focused on recruiting women, one study35 recruited couples. The sample size of populations studied ranged from 3 to 4800 participants.
Study design
All studies were cross-sectional in nature and did not follow participants over time. Eleven studies used comparison groups of women who did not undergo FGM/C7 24–27 29–32 34 35 while five studies reported results only from women who underwent FGM/C.28 33 36–38
Measurement of adverse mental health outcomes
Studies used a variety of instruments for psychological assessment. Four studies used the Hopkins symptoms check list 25 (SCL 25) to assess the burden of depression and anxiety.27 28 33 37 Three studies used the SCL 90 to assess the burden of somatisation, depression, anxiety, hostility and phobia.24 25 32 Three studies used the mini international neuropsychiatric interview to assess either the burden of PTSD, affective disorder, anxiety7 30 or the burden of depression.37 Two studies used the General Health Questionnaire-28 item to assess the burden of somatic symptoms, insomnia, social dysfunction and depression.31 34 Two studies used the Harvard Trauma Questionnaire-30 item to assess the burden of PTSD.28 37
Instruments used in one study to assess the burden of PTSD included the PTSD CheckList-Civilian Version,29 PTSD Inventory,25 Arabic version of Child PTSD Reaction Index26 and PTSD Symptom Scale-Interview.28 Instruments used in one study to assess the burden of depression included the Center for Epidemiologic Studies Depression Scale29 and the Arabic version of the Children’s Depression Index.26 One study used the SCL-25 to assess the overall the burden of mental health disorders.35 Two studies did not provide information on the instruments used for psychological assessment.36 38
Study quality assessment and risk of bias
Studies varied in quality but the majority received a rating of ‘fair’ quality. Only one study received a rating of ‘good’ quality,27 nine studies received a rating of ‘fair’ quality24–26 28 30 31 33 35 37 and six studies received a rating of ‘poor’ quality.7 29 32 34 36 38 Lack of sample size justification, limited assessment of confounding factors (lifetime traumatic events in particular) and lack of outcome stratification based on FGM/C type were the most common limitations. Moreover, the majority of studies did not report on the participation rate of individuals eligible for the study or whether outcome assessors were blinded to the exposure status of participants. We present the detailed quality assessment of each study in online supplementary file 2.
Supplemental material
Among the three types of risk of bias we assessed, studies reported the highest risk of bias in exposure/outcome relationship measurement (eight studies) followed by comparability (four studies), then selection risk of bias (two studies). A rating of ‘unclear risk’ was given to 11 studies when assessing selection risk of bias, 10 studies when assessing comparability risk of bias and 7 studies when assessing exposure/outcome relationship measurement risk of bias. We present the detailed risk of bias assessment of each study in figure 2.

Reviewers' judgement about risk of bias for each item across included studies.
Exposure to lifetime traumatic events
Lifetime traumatic events can confound reported mental health outcomes.39 Yet, only four studies7 25 27 29 explicitly reported on lifetime traumatic events when examining the association between FGM/C and adverse mental health outcomes. Three studies7 25 29 used ‘lifetime traumatic events’ as a demographic variable of study participants. Only one study27 identified ‘lifetime traumatic events’ as a variable predictive of adverse mental health outcomes incorporated in a regression model.
Overall study results
Fourteen out of the 16 studies reported an association between FGM/C and at least 1 adverse mental health outcome7 24–35 37; five of these studies explicitly noted that the results were not statistically significant for all25 29 31 or some outcomes.32 34 Of the remaining two studies, one study36 concluded that there was no association between FGM/C and adverse mental health outcomes and the other study38 did not provide reportable results.
When stratified by study design, 11 studies7 24–27 29–32 34 35 also assessed the burden of adverse mental health outcomes among a comparison group (control group). In eight of these studies,7 24 26 27 30 32 34 35 there was a higher burden of adverse mental health outcomes among women who underwent FGM/C compared with the control group. In the remaining three studies25 29 31 that assessed a control group, the results were mixed, that is, some of adverse mental health outcomes measured were higher among the group that did not undergo FGM/C. Another five studies28 33 36–38 did not use a control group. Among these, three studies28 33 37 reported an association between FGM/C and adverse mental health outcomes.
Study results stratified by mental health outcome
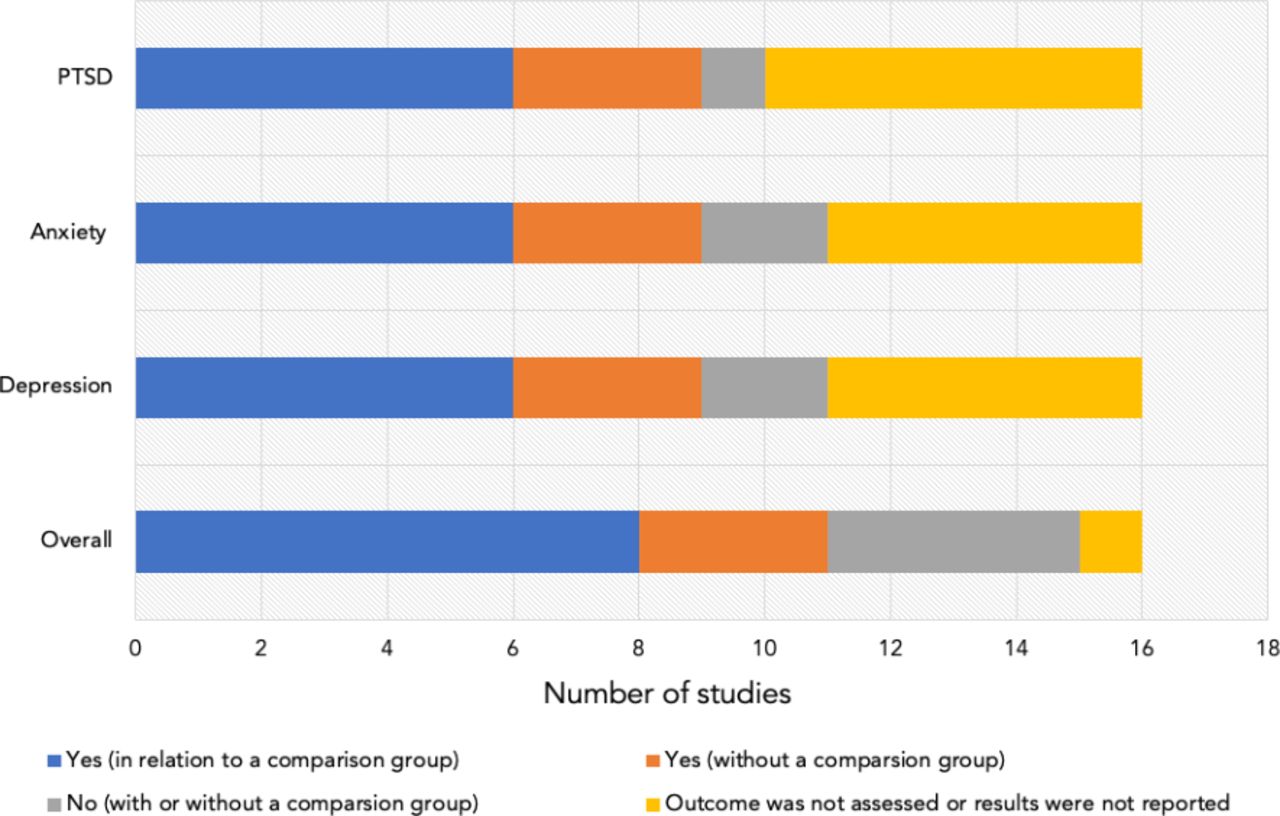
As shown in figure 3, results differed depending on the mental health outcome assessed. Of the 11 studies that assessed depression as an outcome, three studies29 32 34 received a rating of ‘poor’ methodological quality. Six studies24 26 27 31 32 34 reported a higher burden of depression among women who underwent FGM/C compared with the control group of women who did not undergo FGM/C; two of these studies31 32 explicitly noted that the results were not statistically significant. Conversely, two studies25 29 reported a higher burden of depression among women who did not undergo FGM/C; both studies explicitly noted that the results were not statistically significant. Three studies28 33 37 that only assessed women who underwent FGM/C—that is, no control group—reported a high burden of depression among participants.

{kind=link}
{kind=link}
{kind=link}
Overview of studies examining the association between FGM/C and adverse mental health outcomes. FGM/C, female genital mutilation/cutting; PTSD, post-traumatic stress disorder.
Among the 11 studies that assessed anxiety as an outcome, two studies7 32 received a rating of ‘poor’ methodological quality. Six studies7 24 26 27 30 32 reported a higher burden of anxiety among women who underwent FGM/C compared with the control group of women who did not undergo FGM/C. Conversely, two studies25 31 reported a higher burden of anxiety among women who did not undergo FGM/C; both studies noted that their results were not statistically significant. Three studies28 33 37 that only assessed women who underwent FGM/C—no control group—reported a high burden of anxiety among participants; one of these studies33 explicitly noted that the results were not statistically significant.
Of the 10 studies that assessed PTSD as an outcome, one study7 received a rating of ‘poor’ methodological quality. Six studies7 25–27 29 30 33 reported a higher burden of PTSD among women who underwent FGM/C compared with the control group of women who did not undergo FGM/C; among these, two studies25 29 noted that the results were not statistically significant. Conversely, one study31 reported a higher burden of PTSD among women who did not undergo FGM/C; the study explicitly noted that the results were not statistically significant. Three studies28 33 37 that only assessed women who underwent FGM/C—no control group—reported a high burden of PTSD among participants.
Other notable adverse mental health outcomes assessed included somatic symptoms (six studies7 24 26 30 32 34; all reported an association), overall affective disorder (two studies7 30; both reported an association) and overall psychological consequences (three studies35 36 38; one reported an association35).
Study results stratified by geographical location
Of the 10 studies conducted at the participants’ country of origin, three studies7 32 34 received a rating of ‘poor’ methodological quality. Eight of the 10 studies7 24 26 27 30 32 34 35 reported a higher burden of adverse mental health outcomes among women who underwent FGM/C compared with the control group of women who did not undergo FGM/C. Conversely, two studies25 31 reported mixed results, that is, some outcomes were higher among the group that did not undergo FGM/C.
Of the six studies that targeted migrant women, three studies29 36 38 received a rating of ‘poor’ methodological quality. One study29 that compared adverse mental health outcomes between women who underwent FGM/C and women who did not undergo FGM/C reported mixed results. Three studies28 33 37 that only assessed women who underwent FGM/C—no control group—reported a high burden of adverse mental health outcomes among participants. One study36 without a control group reported a lack of association between FGM/C and adverse mental health outcomes and another study38 did not provide reportable results.
Study results stratified by FGM/C type
Four studies27 30 33 37 investigated whether FGM/C type (severity) affected the severity of adverse mental health outcomes. All four studies reported a correlation between the severity of FGM/C and the severity of adverse mental health outcomes. FGM/C type III (the most severe form) had the highest association with adverse mental health outcomes.
Discussion
In a comprehensive review of the literature about the relation between FGM/C and adverse mental health outcome, we found that of the 16 studies included, 14 reported an association between FGM/C and at least 1 adverse mental health outcome. The studies that examined specific mental health outcomes consistently reported an association between FGM/C and that particular outcome. The four studies that stratified their results by FGM/C type found an association between the severity of FGM/C and the severity adverse mental health outcomes. Importantly, our review found that of the included studies only one received a rating of ‘good’ methodological quality. Further, the majority of studies reported ‘high risk of bias’ or ‘unclear risk’ in one or more of the categories used to assess risk of bias.
Our findings are consistent with results of prior smaller reviews. For example, the review by Berg et al (included four studies), reported an association between FGM/C and adverse mental health outcomes. The same review highlighted the lack of rigour in study design and methods in included studies (all studies received a rating of ‘moderate’ or ‘low’ quality).14 In their literature review on the long-term health consequences of FGM/C, Reisela and Creighton concluded that the FGM/C led to long-term adverse psychological outcomes (based on three studies).16 Our review adds to the literature through providing a more comprehensive overview of existing research on adverse mental health outcomes linked to FGM/C. Further, we provide a quality assessment for existing literature on the subject.
This review is not without limitations. First, like all systematic reviews, our review is subject to publication bias. It is possible that studies that did not show an association with mental health outcomes were not published. However, the consistent presence of an association across studies—and the observation of a dose–response relationship between the severity of FGM/C and mental health outcomes in four studies—mitigates the concern that what we are seeing spurious findings due to publication bias. Second, all the studies included in our review are cross-sectional in nature, with a small sample size, and many do not account for confounding factors; lifetime traumatic events in particular. It is, therefore, difficult, from these studies, to isolate causality only to FGM/C and it is not implausible that the observed mental health consequences are attributable to a host of concomitant conditions that disadvantage the women studied. Third, the quality assessment tools we used, while designed for observational studies in general, may be limited when assessing cross-sectional studies. This limitation, however, is more reflective of the lack of proper tools to assess cross-sectional studies in general. Finally, due to the heterogeneity in the psychosocial assessment tools used by the studies, and the low quality of included studies, it was not possible to conduct a quantitative meta-analysis of the results. It is worth noting that these limitations highlight the need to invest in quality longitudinal research on the adverse mental health consequences of FGM/C.
Conclusion
While there is a large body of literature on the physical effects of FGM/C, there is little quantitatively measuring the mental health consequences of the practice. This review provides a comprehensive summary of the existing literature on the adverse mental health consequences of FGM/C. The observation that FGM/C is associated with adverse mental health outcomes should not be surprising. There is abundant evidence that traumatic event experiences are associated with adverse mental health outcomes over the life course.40 FGM/C, especially severe forms, can be a traumatic experience through deliberating inflicting of harm on girls, often without anaesthesia, at a particularly sensitive life course period. This review should set to rest, once and for all, the misconception that the cultural normalisation of FGM/C somehow minimises the adverse mental health consequences associated with this practice.15 This review shows that, in addition to the physical consequence of this practice, it is also associated with poor mental health outcomes that may accompany women throughout their lives.
Importantly, our review demonstrates the need for further, better quality, research on the topic. Based on our review, future research should aim to incorporate the following criteria to improve the methodological quality of evidence on the topic: 1) improve and standardise the psychological tools necessary to assess the association between FGM/C and adverse health outcomes; 2) independently investigate the board range of potential adverse mental health outcomes that may be associated with undergoing FGM/C; 3) stratify reported outcomes based on FGM/C type; 4) address and control for potential confounding, lifetime traumatic events in particular; and 5) use longitudinal study designs to document the full scope of the mental health consequences of FGM/C over time.
References
Footnotes
Handling editor Seye Abimbola
Twitter @SalmaMHAbdalla
Contributors SMA concieved the design of the study. SMA led the analysis process with support and supervision from SG. SMA wrote the first draft and SG commented and edited all versions of the draft. Both authors read and approved the final draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No additional data are available.