Article Text

Abstract
Introduction NAMWEZA is a novel intervention that focuses on preventing HIV and promoting sexual and reproductive health and rights by addressing underlying factors related to vulnerability of acquiring HIV, such as depression, intimate partner violence (IPV) and stigma. The goal of the study was to evaluate the effect of the NAMWEZA intervention on risk behaviour as well as factors potentially contributing to this vulnerability for people living with HIV and their network members.
Methods A stepped-wedge randomised controlled trial was conducted from November 2010 to January 2014 among people living with HIV and their network members in Dar es Salaam, Tanzania. 458 people living with HIV were randomised within age/sex-specific strata to participate in the NAMWEZA intervention at three points in time. In addition, 602 members of their social networks completed the baseline interview. Intention-to-treat analysis was performed, including primary outcomes of uptake of HIV services, self-efficacy, self-esteem, HIV risk behaviour and IPV.
Results For people living with HIV, a number of outcomes improved with the NAMWEZA intervention, including higher self-efficacy and related factors, as well as lower levels of depression and stigma. IPV reduced by 40% among women. Although reductions in HIV risk behaviour were not observed, an increase in access to HIV treatment was reported for network members (72% vs 94%, p=0.002).
Conclusion These results demonstrate the complexity of behavioural interventions in reducing the vulnerability of acquiring HIV, since it is possible to observe a broad range of different outcomes. This study indicates the importance of formally evaluating interventions so that policymakers can build on evidence-based approaches to advance the effectiveness of HIV prevention interventions.
Trial registration number NCT01693458.
- HIV prevention
- people living with HIV
- social networks
- behavioural intervention
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Behavioural interventions to prevent HIV transmission have demonstrated varying levels of effectiveness in resource-limited settings.
In addition to targeting HIV risk behaviour, effective interventions should focus on underlying factors contributing to the vulnerability of transmission, including depression, intimate partner violence (IPV), HIV-related stigma and fear of disclosure of HIV status, among other psychosocial characteristics.
What are the new findings?
People living with HIV who participated in NAMWEZA to serve as Change Agents for HIV prevention in their communities experienced lower levels of depression, stigma and IPV; although reduction in HIV risk behaviours was not observed.
Among social network members of the Change Agents, improvement was observed for self-efficacy for safer sex but not for HIV risk behaviours; an increase in access to HIV testing was marginally significant and improvement in access to HIV treatment was observed for network members that were living with HIV.
What do the new findings imply?
People living with HIV can serve as Change Agents in their communities for HIV prevention as demonstrated by the NAMWEZA intervention; however, their effectiveness can vary based on the targeted outcomes, content of the curriculum and the extent that issues of HIV status disclosure are a concern.
Introduction
Over the past several decades, since its advent, the HIV epidemic has transformed in impact and scope.1 Initially as a disease of impaired immunity with no effective treatment, HIV resulted in high death rates.2 3 With the increasing availability of antiretroviral therapy (ART) the prognosis and survival of HIV improved significantly, where HIV disease can currently be considered a chronic condition.4 Since the expansion in availability of ART in Tanzania in the early 2000s, tremendous strides have been made in prognosis and survival of people living with HIV, similar to what has been observed in other resource-limited settings.5 As a result, a local initiative has promoted ‘Prevention with Positives,’ a programme that focuses on integrating discussion of reducing risk behaviour within the context of HIV-related clinic visits. This programme has engaged lay counsellors to conduct group education sessions on prevention and provided individual counselling sessions with people living with HIV in Tanzania, as well as Namibia and Kenya.6
More broadly, a number of interventions have been developed that focus on promoting sexual and reproductive health and rights among those living with HIV, with the goal of preventing transmission and repeated exposure to the virus among individuals living with HIV. A significant number of studies have been conducted in the USA,7 8 and findings from low/middle-income countries have demonstrated mixed results.9–11 For example, in a prevention intervention among people living with HIV receiving treatment in clinical settings in Thailand a reduction in unprotected sex was observed overall, but not among men who have sex with men. In rural Uganda, people living with HIV who participated in an HIV treatment programme integrating ART and counselling for prevention demonstrated a reduction in unprotected sex by 50% (p=0.004). In contrast, among pregnant women living with HIV in South Africa participating in a prevention programme, an effect on the incidence of sexually transmitted infections was not observed. For the Prevention with Positives intervention, a reduction in the occurrence of unprotected sex was observed for the Tanzanian site, but not for sites in Kenya and Namibia.12
In addition, to a large extent prior interventions have focused more on reducing vulnerability to HIV infection rather than considering potential underlying factors contributing to transmission, such as structural drivers13 14 and psychosocial issues.15–17 Sexual risk behaviour may be affected by a number of psychosocial factors, such as the level of HIV-related stigma, depressive symptoms,18 lack of HIV disclosure,19 limited social support and employment status,20 among other related variables. In particular, HIV-related stigma can reduce social support and exacerbate other psychosocial problems, which can increase the risk of depressive symptoms or result in concerns related to inadvertent disclosure of their HIV status. In addition, these psychosocial factors can also be a result of the larger sociopolitical/economic context that can promote poverty and gender inequality. Considering these issues can allow policymakers and program developers to address some of the root causes of vulnerability of acquiring HIV. This suggests that a more holistic approach to care and prevention services for people living with HIV is warranted. In particular, considering the broader approach of sexual and reproductive health and rights can potentially result in interventions that are more effective for people living with HIV.21
The NAMWEZA intervention was initially developed in Uganda and adapted in Tanzania with the goal of preventing HIV and promoting sexual and reproductive health and rights through fostering affirming relationships between participants and giving rise to a strong sense of relational responsibility; while at the same time working with people living with HIV to become advocates for change in their communities.22NAMWEZA worked with people living with HIV who would focus on protecting themselves, and would reach out to those in their social networks to prevent HIV transmission. Those who participated in the intervention directly (10 weekly group sessions) were people living with HIV, considered to be Change Agents in their communities, and were encouraged to discuss underlying factors that can contribute to the vulnerability of acquiring HIV with members of their social networks. In this regard, we hypothesised that the intervention would have an effect on HIV-related risk behaviour, and on other primary outcomes such as uptake of HIV services, self-efficacy for safer sex, general self-efficacy, self-esteem and intimate partner violence (IPV). Secondary outcomes included HIV knowledge, social support, HIV-related stigma and depressive symptoms. The overall goal of this study was to evaluate the NAMWEZA intervention among the Change Agents and members of their social networks, to examine whether there was an effect on risk reduction, and for these underlying psychosocial risk factors as well.
Methods
Study design
A stepped-wedge randomised controlled trial (RCT)23 was conducted from November 2010 to January 2014 in Dar es Salaam. Among 753 people living with HIV approached, 652 met the initial eligibility criteria: (1) ≥18 years of age; (2) receiving ART for least 3 months; (3) living in Kinondoni municipality; (4) willingness to work with members in their social network as a Change Agent/educator; and (5) willingness to invite up to 10 members in their social network with a high vulnerability of acquiring HIV to participate in baseline and follow-up interviews. Although this group completed the baseline interview, 194 were excluded since they were unable to recruit network members, resulting in 458 being randomised to one of three steps. All baseline interviews were completed by August 2012 and people living with HIV (hereafter referred to as Change Agents) were randomly allocated to receive the NAMWEZA intervention in one of three chronological steps that occurred during the following time periods: (1) September to November 2012; (2) February to April 2013; and (3) August to October 2013. Follow-up interviews occurred subsequent to each step until January 2014 (see figure 1).
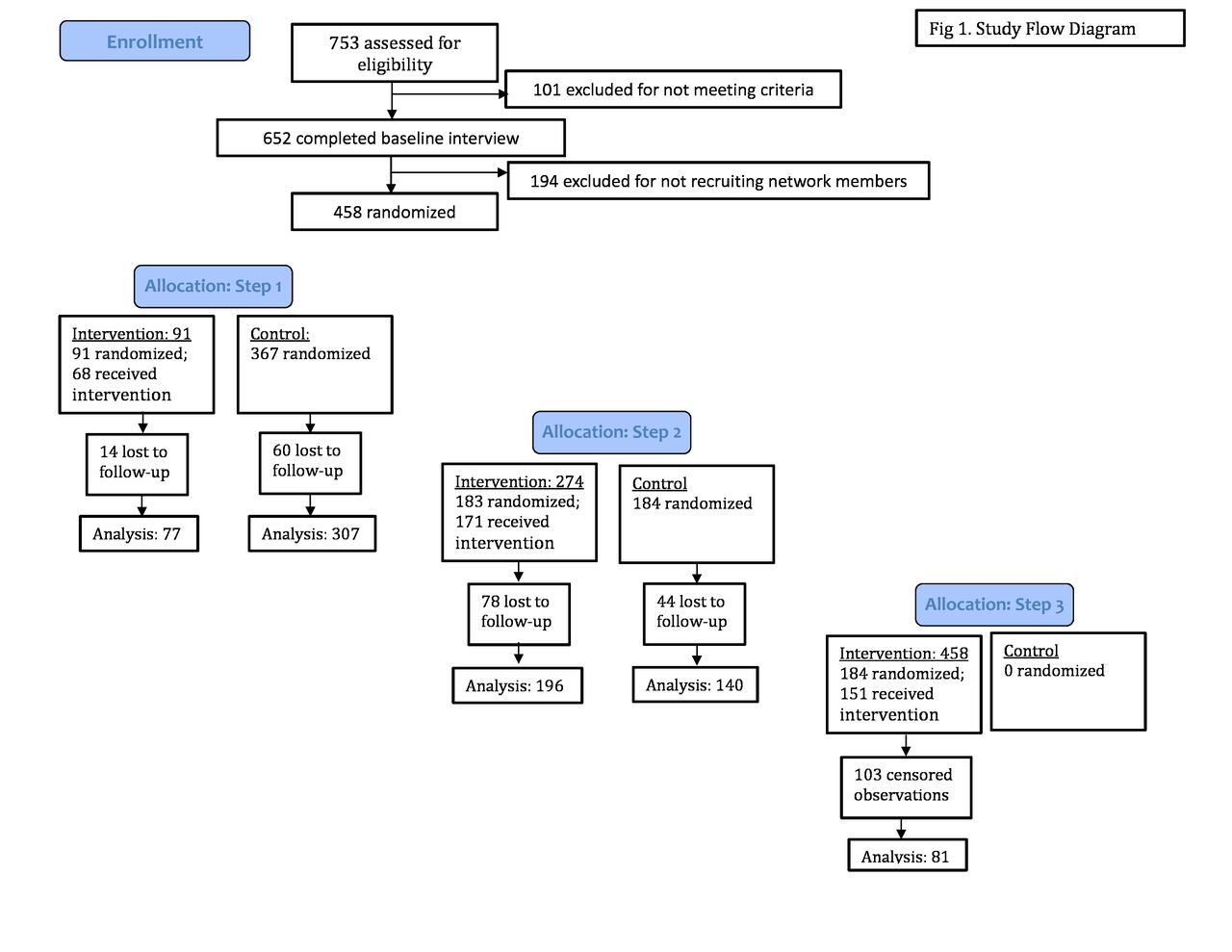
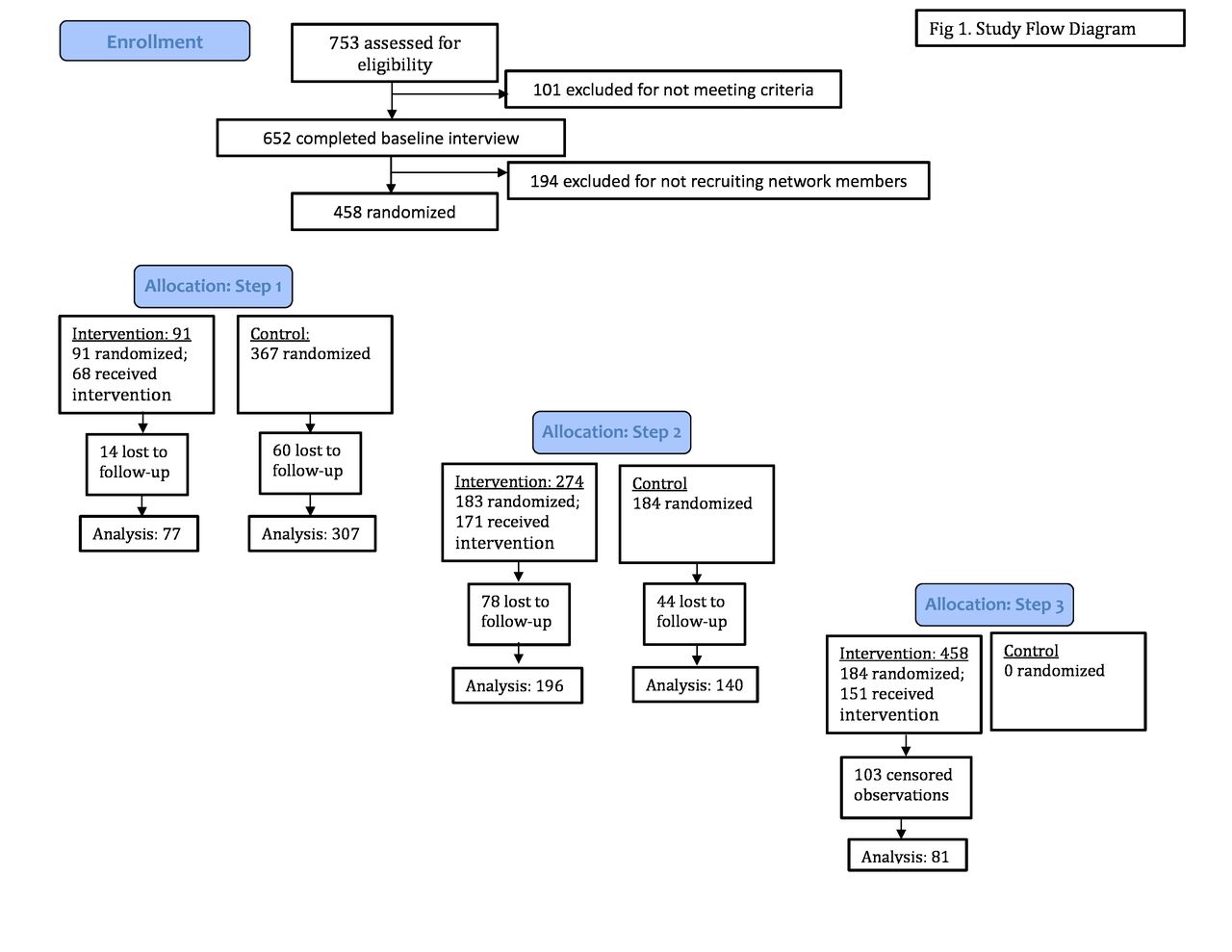{kind=link}
Study flow diagram.
This study design allowed for comparison of Change Agents who randomly received the intervention versus those who had not yet received the intervention at different time periods. Change Agents were initially included in the control group, transitioning to the intervention group after completing the 10 NAMWEZA group sessions. Prior to participating in the group sessions individuals were considered to be part of the control group; after completing the programme they were included in the intervention group. Since it was a behavioural intervention that included group sessions it was not possible to ‘blind’ group facilitators or study participants when a specific group was receiving the intervention. The stepped-wedge design is efficient and more feasible logistically, as it allows the intervention to be phased in over time to include all study participants.
Randomisation of Change Agents was based on four age/sex strata (women <35 years; women ≥35 years; men <40 years; men ≥40 years) since the intervention involved group sessions with a focus on engagement and participation. Within the local context, relatively homogeneous age/sex groups would lend itself to greater participation and interaction within the sessions. The higher age range for younger men to include those less than 40 years was based on findings from prior qualitative work, where younger women were often partners with men who were older on average. Within each age/sex stratum, prospective study participants (Change Agents) were assigned a random number. A random number generator was then used to determine if participants would be allocated to steps 1, 2 or 3 at a 1:2:2 ratio to ensure fidelity of the intervention during the first step of the study. The Program Manager generated the random allocation sequence and implemented the random assignment of participants. The Principal Investigators were not involved in randomly allocating study participants to the three steps. Change Agents were encouraged to reach out to members of their social networks to share what they learnt in the intervention and promote sexual and reproductive health and rights as well as HIV prevention in their communities.
Study population and implementation
The study was conducted within the context of two government HIV care and treatment centres (CTC) located in one municipality of Dar es Salaam, Tanzania, that provided treatment to more than 5000 patients living with HIV per year. People living with HIV were recruited through distribution of fliers and more detailed information sheets about the study with staff inviting individuals in the waiting rooms of the two HIV clinical sites. People living with HIV were considered Change Agents and participated in 10 group sessions through the NAMWEZA intervention (see the Intervention section). Through the sessions, Change Agents were trained to reach out to members of their social networks (Network Members) to discuss HIV prevention and sexual health as well as promote access to services, including HIV testing. Once enrolled, each Change Agent was asked to invite up to 10 Network Members to participate in a general health education programme called ‘Text4Health’, which involved the completion of baseline and follow-up questionnaires and the receipt of health education-related text messages. The Network Members were enrolled in step 1 (n=129), 2 (n=241) or 3 (n=232) based on the assigned step of their Change Agents. The mean number of Network Members for the Change Agents was 2 (SD=0.66; range 1–4). To prevent inadvertent disclosure of HIV status of the Change Agents, the Network Members completed the questionnaires at a different location unrelated to HIV services in the same municipality.
Inclusion/exclusion criteria
For Change Agents, the inclusion criteria for the trial were: (1) the initial eligibility criteria outlined above; (2) completing a baseline interview; and (3) attending a reorientation session. Change Agents not well enough to attend the training sessions at baseline were excluded. Inclusion criteria for the Network Members were: (1) 18 years of age or above; and (2) being invited by a Change Agent to participate in the study. Network Members were excluded if they were: (1) receiving HIV care and treatment services at the study clinics; or (2) already invited by another Change Agent.
Recruitment and retention
From the two recruitment sites, 753 individuals were approached to participate in the study and 87% were eligible. Change Agents who were not able to recruit network members due to personal time constraints or out of fear of disclosing their HIV status were excluded from randomisation. Reorientation sessions were offered to the Change Agents to discuss strategies for approaching those in their networks for participation. The 458 individuals who attended reorientation sessions were randomised to participate in the trial (see figure 1). For the Change Agents who were randomised, 602 of their Network Members participated in the study at baseline. Throughout recruitment and follow-up, appropriate referrals for treatment were implemented by programme staff on an as needed basis. For any potential of harm (self-harm or harm to others) to study participants, referrals were made to medical facilities and specialised assistance for gender-based violence.
The retention of Change Agents is shown in figure 1 (73%) at step 2. Due to limitations in study resources, after completion of the 10 group sessions for step 3, only 81 Change Agents were followed up with a final interview for this last step. For Network Members, retention at follow-up was 62%. The primary reason for lack of study retention was that the participant either moved and/or changed his/her telephone number and could no longer be located. Other reasons included participants’ competing responsibilities at work and home as well as travelling out of town for extended periods of time.
Intervention
The NAMWEZA (meaning ‘Yes, together we can!’) programme is based on an appreciative inquiry framework.24 A more detailed description of the intervention is provided by McAdam et al.22 Although this approach has been used more commonly in business and other settings with focus on fostering organisational change, it has been used recently within psychotherapeutic, family and community initiatives as well as health interventions.25 The appreciative framework is linked with a positive psychology theoretical approach, since it relates to exploring the development of hope and future-mindedness and focusing on self-efficacy and an affirmative perspective of the future.26 The initial curriculum was created from a psychotherapeutic perspective with many experiential exercises included to create relationships of competence between participants and to have a future orientation in which participants could dream and create ideas for their future lives. Dr Alice Welbourn, Stepping Stones developer, was invited to collaborate in the initial curriculum development and contributed some of the content of the Stepping Stones intervention27–29 which has been used throughout sub-Saharan Africa, including Tanzania. This allowed the appreciative inquiry approach to be integrated into an evidence-based platform for HIV prevention in sub-Saharan Africa that focused on reducing risk behaviours and addressing the structural drivers of HIV transmission.
Prior to study implementation adaptation of the appreciative inquiry framework to the local context occurred in active discussion with lay counsellors at community-based organisations (CBO) in Dar es Salaam. These discussions also occurred within the context of adapting the manual and during the translation process. The overall approach corresponded well with the experiential learning and feedback strategies of the intervention. The NAMWEZA framework focused on HIV prevention from the perspective of engaging participants in creating relationships through a sense of pride and competence by identifying positive skills and qualities in each other as well as others within their social networks. In addition, the development of social cohesion within the groups is consistent with what is known about the strength of peer support in HIV-related interventions.30–32
Based on this premise, the implementation process in all sessions explored different communication strategies and abilities of people that would facilitate positive images of the future. Each session began with an appreciative inquiry exercise, discussing different aspects of their lives and what they were learning in the intervention. The content of the 10 weekly sessions comprised: (1) introduction that included setting the ground rules/ethics for the sessions; (2) love, relationships and feelings; (3) valuing different perspectives, valuing ourselves, valuing our bodies; (4) happy, healthy, safer sexual relations; (5) developing our assertiveness skills; (6) deepening and expanding our assertiveness skills; (7) disclosure (part 1); (8) disclosure (part 2); (9) exploring income-generating skills; and (10) the future. The sessions were based on a structured curriculum; however, the focus was participatory in nature to encourage discussion and interaction among the group members. See box 1 for a detailed outline of the intervention.
NAMWEZA intervention outline
Session 1: Introduction—setting ground rules and expectations for participation in NAMWEZA, creating an environment built upon trust and confidentiality.
Session 2: Love, relationships and feelings—exploring the value of love, understanding emotions and how they can impact communications within relationships.
Session 3: Valuing different perspectives, valuing ourselves, valuing our bodies—learning to value our own and others’ perspectives, understanding how our values inform our decisions.
Session 4: Happy, healthy, safer sexual relations—exploring and developing knowledge about sexual relations and HIV, encouraging participants to share their knowledge and competencies.
Session 5: Developing our assertiveness skills—focusing on assertiveness and taking control of our bodies and ourselves, practising how to address problems without antagonising or withdrawing from people.
Session 6: Deepening and expanding our assertiveness skills—exploring different responses to difficult situations, recognising participants’ communication skills and sharing strategies and skills with others.
Session 7: Disclosure (part 1)—reflecting on their experiences and considering the issue of disclosure of one’s HIV status, anticipating and addressing responses of people with whom you may wish to disclose.
Session 8: Disclosure (part 2)—experiencing role plays and practising different approaches to disclosure with partners and other loved ones.
Session 9: Exploring income-generating skills—reflecting on the link between skills and resources in terms of creating potential income-generating possibilities.
Session 10: The future—considering the role of dreams about the future and their roles as advocates.
The group sessions were held once a week for 10 consecutive weeks and were 3–3.5 hours in length, for a total number of 30–35 hours for the intervention. They were held in a primary school adjacent to the main healthcare centre for the study and were facilitated by four trained community-based health workers (CBHW) matched by age/sex groups, with approximately 20 individuals in each group. The lay providers who served as the group facilitators were recruited from CBOs based in Dar es Salaam working with people living with HIV who were also providing counselling services. Within the CBOs, we selected providers who specifically had demonstrated a respect for others, a sense of optimism and experience with counselling among people living with HIV. Additionally, we recruited individuals who were living with HIV, had been directly affected by the HIV epidemic on a personal level and had successfully navigated HIV care and treatment services with good treatment outcomes.
Training was directly provided by the developers of the NAMWEZA intervention. This involved an intensive 2-week training, where lay providers actively participated in each of the NAMWEZA sessions, which were facilitated by the trainers. This was followed by weekly sessions over 2 months to advance comprehension of the intervention manual, understand the links between sessions, strengthen skills for active learning and participate in a pilot to gain experience with appreciative facilitation strategies.
Self-evaluation reporting tools were drafted by CBHWs and included detailed notes reflecting on their experiences facilitating the groups on a weekly basis, which were reviewed with their supervisors. Fidelity of the intervention was strengthened through meetings of lay providers with their supervisors on a weekly basis. In addition, the CBHW supervisors would often cofacilitate sessions with the CBHWs. Adequate staffing also ensured that two to four facilitators were available for every session. Lastly, a research assistant conducted observations of implementation of the first, fifth and final sessions that examined content covered, confidence in delivery, levels of participation and duration of sessions.
Data collection and measures
Structured questionnaires were approximately 2 hours long and were administered using Audio Computer-Assisted Self-Interview (ACASI) software for assessment at baseline and three follow-up visits coinciding with the completion of a subsequent Change Agent training wave. Due to logistical constraints in contacting Network Members, only one follow-up assessment was feasible. The questionnaires included items used for HIV clinical care at CTCs in Dar es Salaam for sociodemographic characteristics and uptake of HIV testing or care services.33 34
For the primary outcomes, the ACASI questionnaire included validated questions and scales used in a number of different settings. The General Self-Efficacy Scale assessed one’s overall confidence in coping with a range of stressful situations35; it has demonstrated validity in a number of cultural contexts.36 37 Self-efficacy for safer sex was based on the Condom Use Self-Efficacy Scale, which demonstrated good reliability and validity in Ghana. This measure focused on the extent one was confident in using condoms consistently and negotiating safer sex.38 Self-esteem was assessed using the Rosenberg Self-Esteem Scale, which has an estimated Cronbach’s alpha ranging from 0.77 to 0.88 and has demonstrated associations with anxiety and depression.39 IPV was measured using the Domestic Violence module of the Tanzania Demographic and Health Survey,40 including victimisation and perpetration of sexual as well as physical violence. We also included relevant items from a questionnaire used by the Prevention with Positives study in Tanzania that assessed comparable outcomes, including access to HIV testing and services, multiple sex partners as well as unprotected sex.
Additionally, for secondary outcomes a number of items from other existing measures that have demonstrated validity and reliability were used, including depressive symptoms (Patient Health Questionnaire-9 [PHQ-9]),41 HIV knowledge,6 social support42 and HIV-related stigma.43
Sample size calculations
For the sample size calculations, the study was powered for three primary outcomes: uptake of HIV services among Network Members, unprotected sex and IPV. For network members, the power calculations assumed an alpha level of 0.05, a baseline prevalence of 10% and an OR of at least 1.5 for the uptake of HIV services to reach a power of 80%. In addition, assuming that at baseline 38% of network members and Change Agents had unprotected sex and an alpha level of 0.05, the study had greater than 80% power if the OR estimates were 0.70 or lower. The study also achieved 80% power to observe a reduction in prevalence of IPV, assuming a baseline rate of 30%, an alpha level of 0.05 and an OR of 0.70. These calculations accounted for 85% and 80% retention rates for Change Agents and Network Members, respectively.
Statistical analysis
Descriptive statistics were calculated for sociodemographic variables as well as primary and secondary outcomes at baseline and follow-up. Intention-to-treat analyses were performed. The probability of an event at a visit was compared between intervention periods and control periods by using generalised estimating equations, accounting for correlation within an individual’s outcomes at different times. Risk ratios (RR) and 95% CIs were reported. Likewise, for continuous outcomes, we compared group means from intervention periods to control periods by using generalised estimating equations. Analyses for Change Agents were stratified by sex since the intervention was administered separately.
For the Network Members, since we only have one follow-up interview for the majority of Network Members in the sample and they were considered already being ‘intervened’ at the time of follow-up interview, a stepped-wedge RCT analysis was no longer appropriate. The Student’s t-test and χ2 test were used to compare the distribution of outcomes before and after the intervention. Statistical analysis was conducted using SAS software, V.9.3.
The primary outcomes of the study included four domains: (1) unprotected sex and having multiple sex partners among Change Agents and their Network Members; (2) risk of IPV in the Change Agents and their Network Members; (3) levels of self-esteem, self-efficacy, and self-efficacy for safer sex among Change Agents; and (4) uptake of HIV services among the Network Members. HIV services uptake, unprotected sex, multiple sex partners and IPV were explored as binary outcomes. Uptake of HIV services was measured by whether or not the Network Member had accessed HIV testing. For those Network Members who were living with HIV at baseline, accessing HIV care at a CTC was examined. Unprotected sex was defined as anything other than using a condom ‘all of the time’ within the past 6 months. Having multiple sex partners was defined as having more than one partner in the past 6 months. IPV was analysed as any occurrence of physical and/or sexual abuse in the past 6 months, for perpetration and victimisation. Self-esteem, self-efficacy, and self-efficacy for safer sex were explored as continuous outcomes; scores were on a 4-point scale1–4 with higher scores reflecting greater levels of self-esteem, self-efficacy, and self-efficacy for safer sex.
Secondary outcomes included depressive symptoms, social support and HIV-related stigma among Change Agents; and HIV knowledge among Change Agents and their social networks. HIV knowledge was defined as the percentage of correct responses; the mean score was calculated for the analysis. All other secondary outcomes were analysed as continuous variables. Similar to self-efficacy and self-esteem, social support was scored on a 4-point scale,1–4 with higher scores demonstrating greater levels of social support. HIV-related stigma was scored on a 5-point scale,1–5 with higher scores indicating greater stigma. In addition, for depressive symptoms, the PHQ-9 was also scored on a 4-point scale (0–3) with higher scores reflecting a higher level of depressive symptoms.
Ethical and administrative considerations
The study was approved by the Institutional Review Boards at the Harvard T H Chan School of Public Health, Muhimbili University of Health and Allied Sciences, and the National Institute for Medical Research in Tanzania. These approvals are consistent with the principles outlined in the Declaration of Helsinki. In addition, the US Centers for Disease Control and Prevention reviewed the protocol to ensure the protection of the rights of study participants. All participants provided written informed consent.
Results
Among 753 Change Agents approached, 652 were eligible to participate and completed the baseline interview (87%). To support study participants in recruiting Network Members, Change Agents were asked to participate in a reorientation session; 458 Change Agents attended this session and were randomised to steps 1, 2 or 3 (70%). After step 1, a total of 384 participated in the follow-up interview (84%). Subsequent to step 2, a total of 336 participated; therefore, according to the stepped-wedge trial design, overall follow-up rate was 73%. Eighty-one participants had an additional follow-up interview after step 3. The study was censored at the end of January 2014 given the limited duration and resources available for follow-up (see figure 1). In terms of actual participation in the group sessions, 68, 171 and 151 individuals were included in steps 1, 2 and 3, respectively. The average number of sessions attended was 7 (SD=3.43).
Regarding baseline characteristics of the Change Agents, 57% were women and 52% were married or living with a partner. Among women, 54% were under 35 years old; for men 48% were under 40. Younger (60%) and older men (71%) were more likely to be married or cohabiting compared with younger (44%) and older women (52%) (p<0.05). Differences were also observed for employment status, where younger women (32%) and men (47%) reported higher rates of unemployment compared with older women (22%) and men (18%) (p<0.05). Overall, 20% reported problems with food insecurity. In comparing baseline characteristics for Change Agents, frequencies were fairly comparable across intervention groups, with one exception for household lighting. When stratifying by sex, source of household lighting was different across the three steps for men and women (p<0.05). However, no significant differences were observed for other sociodemographic factors (see tables 1A,B).
Baseline sociodemographic characteristics for steps 1, 2 and 3—men (n=197)
Baseline sociodemographic characteristics for steps 1, 2 and 3—women (n=261)
For Network Members, 55% were women and 53% were married or cohabiting. In terms of employment status, 26% of men and 34% of women were unemployed (p<0.05). In addition, a lower rate of food insecurity was also observed for Network Members (10%) as compared with the Change Agents (p<0.05). Other baseline sociodemographic and economic characteristics are described by Kaaya et al.44
Outcomes
For Change Agents, a number of primary outcomes differed significantly before and after their participation in the NAMWEZA intervention, including higher self-esteem, self-efficacy, and self-efficacy for safer sex. Variation was observed for men and women for IPV—physical abuse victimisation demonstrating a reduction in risk among women (RR=0.60; 95% CI 0.38 to 0.94), but not among men (0.77, 95% CI 0.40 to 1.47). Having multiple sex partners in the past 6 months appears to have increased for men and women; however, no changes were observed for unprotected sex. For secondary outcomes, social support for men and women increased. In addition, levels of depressive symptoms and HIV-related stigma declined for both groups, with women experiencing a slightly greater reduction in stigma (−0.37; 95% CI −0.47 to 0.26) compared with men (−0.33; 95% CI −0.45 to 0.21) (see tables 2A,B).
Effect of the NAMWEZA intervention on primary and secondary outcomes for Change Agents—men
Effect of the NAMWEZA intervention on primary and secondary outcomes for Change Agents—women
For primary outcomes among Network Members, an increase in self-esteem was observed (p=0.04); however, no change was observed for self-efficacy or self-efficacy for safer sex. Regarding IPV, physical abuse victimisation also declined (16% to 10%; p=0.003). In addition, no improvements were observed for unprotected sex or number of sex partners. Although there was a marginally significant increase in having an HIV test (74% vs 79%; p=0.06). An improvement in access to HIV treatment was observed for participants who were living with HIV (72% vs 94%; p=0.002). For the secondary outcome analysed for Network Members, HIV knowledge was higher after the intervention (p=0.006).
Some variation was observed when the Network Members were stratified by sex. In particular, improvement in HIV knowledge became marginally significant. Although self-esteem did not improve in the stratified analysis, women experienced a marginally significant increase in self-efficacy. A comparable finding for self-efficacy among men was not observed. Similar to findings from the Change Agents, physical abuse victimisation decreased among women, but not among men. In contrast, men experienced a marginally significant increase in access to HIV testing; however, this was not observed for women. Similar to the aggregated analysis, men and women who were living with HIV among the Network Members reported an increase in access to HIV treatment, although the finding was marginally significant among men (see tables 3A,B).
Effect of the NAMWEZA intervention on primary and secondary outcomes for Network Members—men
Effect of the NAMWEZA intervention on primary and secondary outcomes for Network Members—women
Discussion
Findings from the present study indicate that the NAMWEZA intervention improved self-esteem, general self-efficacy, self-efficacy for safer sex and social support, as well as reduced HIV-related stigma, and depressive symptoms among people living with HIV engaged in clinical care. In particular, reported physical abuse victimisation was reduced by 40% among women who received the intervention compared with the controls. It is also demonstrated that having more than one sex partner in the past 6 months increased for men and women, while unprotected sex remained consistent for intervention and control groups. Additionally, although changes observed for continuous variables may not appear to be large in magnitude, improvement in factors such as HIV-related stigma and depression can have a significant effect on overall quality of life and well-being.
For Network Members, HIV knowledge and self-esteem appeared to improve overall. Similar to the Change Agents, physical abuse victimisation declined; however, in stratified analysis this was only observed among women. In addition, the proportion of members reporting unprotected sex remained high. The prevalence of having multiple sex partners remained consistent over time (62% vs 58%). For HIV-related outcomes among Network Members, a marginally significant improvement in accessing an HIV test for those who were negative at baseline was observed; for those who were living with HIV, an increase in accessing HIV treatment occurred. Similar to this study’s findings, the IMAGE program in South Africa demonstrated an increase in HIV testing among study participants.45
There are a number of factors that can impact the effectiveness of HIV prevention or sexual and reproductive health interventions, including the content and/or duration of the intervention, study design, length of time of follow-up, assessment of outcomes, the study population (eg, women vs men; youth vs adults, HIV status) and methodological limitations. In particular, the local context and the degree of fidelity to the original intervention may play a role. For example, mixed findings were observed for evaluation of the Stepping Stones HIV prevention intervention in different resource-limited contexts.46 The initial study by Jewkes et al in South Africa demonstrated significant improvements in HIV knowledge, condom use, multiple partners and IPV. Although HIV incidence did not decline, the occurrence of herpes simplex virus-2 was reduced over the course of the study.47 However, varying levels of effectiveness were observed for implementation of the Stepping Stones intervention in different resource-limited settings. A reduction in IPV was observed in the Gambia, Tanzania and Fiji; however, no change for this outcome was observed in Angola, Uganda or India. In addition, a decrease in multiple partners was observed in Ethiopia, but not in India. Variation by country was also observed for condom use and factors related to gender equity. Interestingly, a consistent finding across all studies was the improvement in skills to discuss sex with one’s partner, HIV knowledge, as well as reduction in HIV-related stigma. Another consideration is the limitation in quantitative data in capturing complex phenomena; for example, while the quantitative findings in Angola and Uganda did not demonstrate a reduction in IPV as indicated above, qualitative data supported positive changes in men’s behaviour and attitudes towards women.48
In rural Malawi, HIV knowledge, self-efficacy for safer sex and HIV-related stigma also improved among adults participating in a six-session HIV prevention intervention. Although partner communication and condom use increased, no effect was observed for behaviours related to HIV transmission. Similar to findings for the Network Members in the present study, access to HIV testing increased over a 12-month period.49 In Uganda, a community mobilisation intervention to reduce the occurrence of IPV and HIV acquisition (SASA!) resulted in increased discussion with one’s partner about using a condom as well as actual condom use in the past year, although the latter was marginally significant.50 For men in particular there was a significant increase in using a condom during last sexual intercourse. Similarly, having multiple partners was reduced, but only among men. Both men and women reported an increase in joint decision-making in their relationships.
Variability in safer sex was also observed in the Prevention with Positives study, where a reduction in unprotected sex was demonstrated for study clinics in Tanzania, but not in Namibia or Kenya. Among female sex workers exposed to a community-based HIV prevention intervention in Zimbabwe, improvement in consistent condom use was observed for their regular partners; however, this change in behaviour was not transferred to their clients.51 Differences were also observed for other studies of social support group HIV prevention interventions with adolescents/young women living with HIV facilitated by trained lay providers—although no significant difference in sexual transmission behaviour score was demonstrated for intervention versus control groups in a study conducted in Uganda,52 a statistically significant increase in condom use was observed in a similar study in South Africa.53
Limitations
There are a number of limitations in the present study. Given the study design was a stepped-wedge RCT, it was not possible to implement a double-blind study. We anticipate that this has not resulted in bias since we have trained study staff to be aware that it was unclear if the NAMWEZA intervention would be beneficial, which necessitated the RCT design. There is also the potential for contamination across study steps to bias results towards the null. However, contamination was prevented to some extent through the random assignment of individuals to each ‘step.’ Although intent-to-treat analysis was performed, only 85% of those assigned to receive the intervention across the three steps attended at least one session. However, we do not anticipate that this had an effect on the results, since baseline characteristics were comparable for those who were randomised overall and those who participated in the intervention (see online supplementary appendix table S1).
Supplemental material
Limited retention of study participants over time may potentially bias our findings. This may be more of a concern for the Network Members as compared with the Change Agents, since the Network Member follow-up rate was 62% vs 73% for Change Agents. Another limitation related to the Network Members is the pre-post analysis, since only one follow-up visit was feasible. In this regard, unknown confounding variables related to non-intervention-related changes over time may have affected our findings for the Network Members; however, we do not anticipate any other factors outside of those who were controlled for that would have affected the outcomes over the study period. Due to this revision in the analysis strategy for the Network Members, RRs and ORs could not be computed and the relative change was calculated using t-tests for continuous variables and χ2 tests for categorical variables. In addition, small sample size for a number of outcomes could bias results towards the null; there was also inadequate statistical power to examine effect modification by variables other than sex, such as age and HIV status of the network members. It is also possible that null findings might be related to the relatively short intervention time of 30–35 hours, in comparison to similar interventions of longer duration.54 55
The increase in the 6-month prevalence of multiple partners may also be related to a potential change in partner, particularly in the context of a relationship affected by IPV. Since we are not able to determine in the past 6 months the degree of overlap in relationships, it is not clear if concurrency is increasing or only the number of partners is being affected. An alternative interpretation is that increases in self-esteem and self-efficacy may be contributing to the increase in the per cent with multiple partners. Preliminary analysis of qualitative data from in-depth interviews with participants in the intervention suggests that NAMWEZA did have an overall effect on protective behaviours, such as prevention of IPV and safer sex. This suggests that the findings may in part be related to a social desirability bias, that is, that participants were less likely to disclose behaviours related to HIV transmission at baseline compared with after exposure to the NAMWEZA intervention in the quantitative assessment. Future studies should evaluate more closely whether relationships are occurring at the same time, or sequentially, which may differentially affect the level of behaviours related to HIV transmission. Subsequent research should also focus on the potential effect of participating in the programme with your partner as well as the consideration of whether or not participants preferred to get pregnant or have more children. Community-based participatory research using a sexual and reproductive health and rights approach could shed light on potential mechanisms of effect for different outcomes of the NAMWEZA intervention.
Additionally, given the finding on reduction in physical IPV, future studies should inquire about emotional/psychological IPV since this was beyond the scope of the present study. Given that the study participants were recruited from patients actively receiving HIV care, generalisability to the broader population of people living with HIV in Tanzania is limited. However, given increasing access to HIV treatment in Dar es Salaam, patients accessing care are increasingly representative of people living with HIV overall. Lastly, generalisability may also be limited to similar contexts in sub-Saharan Africa.
Conclusion
The NAMWEZA intervention demonstrated a number of outcomes that can improve health and quality of life among the Change Agents and their Network Members, as indicated by reductions in IPV and an increase in self-esteem. Improvements for Change Agents were also observed for self-efficacy, self-efficacy for safer sex, social support, depression and HIV-related stigma. Change Agents also demonstrated an increase in having multiple partners, which can confer a greater risk of acquiring different strains of HIV or other sexually transmitted infections, but may also be a reflection of increased self-esteem. For Network Members, access to HIV testing improved, although this was marginally significant and was only observed among men in the stratified analysis. In addition, Network Members who were living with HIV demonstrated an increase in access to HIV treatment. Although examining clinical outcomes was beyond the scope of this trial, an observational study comparing people living with HIV in NAMWEZA with those who did not participate demonstrated an increase in weight and greater treatment retention at follow-up among those in the programme.56 This finding supports a fundamental goal of the NAMWEZA programme— to improve the overall health and well-being of people living with HIV, which in turn strengthens their capacity to serve as Change Agents in their communities.
The results of this trial add to the evidence base on sexual and reproductive health and prevention interventions for people living with HIV and suggest that treatment settings are feasible for empowering people living with HIV to be Change Agents within their social networks. These findings reflect the complexity of behavioural interventions to reduce the vulnerability of acquiring HIV. The results from this study demonstrate the importance of evaluating HIV prevention interventions in different contexts, allowing those in policy and programme-related positions to make informed decisions. Drawing on evidence-based interventions can potentially advance the effectiveness of sexual and reproductive health and rights programming for people living with HIV and those in their social networks in resource-limited settings. Future implementation research can shed light onto the feasibility and cost of scale-up as well as the potential long-term impact of the NAMWEZA intervention.
Acknowledgments
We express our sincere gratitude to the study participants and to staff related to this study as well as at implementing HIV CTCs who made this study possible. We make a special acknowledgement for Dr Gilly Arthur, in memoriam, a central collaborator from the US Centers for Disease Control and Prevention (CDC) in Dar es Salaam, Tanzania.
References
Footnotes
Handling editor Seye Abimbola
Contributors MCSF conceptualised and designed the study, drafted the initial version of the manuscript, participated in the statistical analysis and interpreted the findings. HS participated in drafting the manuscript, directed the study activities in the field and interpreted the findings. NL, JL and YL participated in drafting the manuscript, conducted the statistical analysis and interpreted the findings. KM, EM, KO, SH, JT and SK conceptualised and designed the study, participated in drafting the manuscript and interpreted the findings. DA participated in drafting the manuscript, managed field operations and interpreted the findings. MS, NM and SM participated in drafting the manuscript, collected data in the field and interpreted the findings. IA and AS participated in drafting the manuscript, assisted in directing the study activities in the field and interpreted the findings. All authors agree to be accountable for all aspects of the work in terms of accuracy and integrity and have approved the final version of the manuscript as submitted.
Funding This research study was funded by the US Centers for Disease Control and Prevention (CDC) (Grant No: TZ/UG.08.0147). Technical and professional staff at the US CDC provided input into the study design and analysis for this manuscript. YL was supported by the UTHealth Innovation for Cancer Prevention Research Training Program Predoctoral or Postdoctoral Fellowship (Cancer Prevention and Research Institute of Texas, Grant No RP160015) at the time of submission.
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the Cancer Prevention and Research Institute of Texas.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Institutional Review Boards (IRB) at the Harvard T H Chan School of Public Health (HSPH), Muhimbili University of Health and Allied Sciences (MUHAS) and the National Institute for Medical Research (NIMR) in Tanzania.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data are freely available from the corresponding author based on request.