Article Text

Statistics from Altmetric.com
Summary Box
In India, a multipronged strategy including large scale programmes, effective capacity building initiatives, strong partnerships, community-based action, and strategic mass media communication led to an increase in the rates of early initiation of breastfeeding from 24.5% in 2006 to 44.6% in 2014 (i.e. a 1.8-fold increase).
In the seven states of India with the highest burden of neonatal mortality, the combined rate of early initiation of breastfeeding increased from 12.5% in 2006 to 34.4% in 2014 (i.e. a 2.7-fold increase).
But there is room for further improvement – in 2014, 81.1% of deliveries were attended by a skilled health provider, while only 44.6% of newborns were breast fed within 1 hour of birth, indicating that rates of early initiation of breast feeding could double if all newborns delivered by a health provider were breast fed within 1 hour of birth.
There is an urgent need to continue to strengthen national and state policies, hospital and maternity practices, and the knowledge and skills of birth attendants—physicians, midwives and nurses—to support early initiation of breast feeding as a key component of essential newborn care.
In India, 1.2 million children aged 0–59 months die yearly. An estimated 58% of these deaths occur during the neonatal period (ie, the first 28 days of life).1 A meta-analysis of three large trials conducted in Ghana, India and Nepal found that early initiation of breast feeding was associated with a 44% lower risk of neonatal mortality (RR 0.56; 95% CI 0.40 to 0.79).2–5 More recently, analyses on a large cohort of almost 100 000 newborns from three large trials in Ghana, India and Tanzania has shown that, compared with infants who initiated breast feeding within the first hour of life, the risk of neonatal death among children who initiated breast feeding between 2 and 23 hours after birth was 41% higher (RR 1.41; 95% CI 1.24 to 1.62), and 79% higher among those who initiated breast feeding at 24–96 hours of birth (RR 1.79; 95% CI 1.39 to 2.30).6 Therefore, supporting mothers to initiate breast feeding within 1 hour of delivery is a proven high-impact intervention for neonatal survival.7 ,8
In 2006, India's National Family Health Survey indicated that only 24.5% of newborns were breast fed within 1 hour of birth as recommended by India's Ministry of Health and the WHO. Furthermore, in Bihar, Chhattisgarh, Jharkhand, Madhya Pradesh, Odisha, Rajasthan and Uttar Pradesh—the seven states where 55% of Indian infants were born and 64% of newborn deaths occurred—the combined rate of early initiation of breast feeding was a mere 12.5%.9
Since 2006, the Government of India and India's state governments—with technical support from UNICEF and other partners—have been implementing a comprehensive eight-pronged strategy to support breast feeding: (1) incorporating outputs and budgets to support breast feeding in the annual implementation plans of India's flagship programmes for child health, nutrition and development, namely the National Health Mission and the Integrated Child Development Services, the largest of their kind in the world;10 ,11 (2) mainstreaming support for early initiation of breast feeding in the scale-up of Janani Suraksha Yojana, the national conditional cash transfer programme to increase births in health facilities and reduce maternal and neonatal deaths;12 (3) ensuring support for breast feeding in special newborn care units, which provide care for sick newborns with birth asphyxia, jaundice, sepsis or low birth weight;13 (4) forging alliances with training colleges, medical schools and professional bodies such as the Indian Academy of Paediatrics to mainstream breast feeding into the pre-service curricula of health professionals;14 (5) building the capacity of practising physicians, midwives and nurses to ensure that women who deliver in a health facility are supported to breast feed within 1 hour of birth;15 (6) strengthening the capacity of community frontline workers of the National Health Mission and the Integrated Child Development Services programmes to provide mothers—during and after pregnancy—with counselling on and support for optimal breast feeding;16–18 (7) mainstreaming support for breast feeding in the work of grassroots women's groups and non-governmental organisations to promote positive behaviour and social change for breast feeding; and (8) communicating the benefits of breast feeding through large-scale media campaigns.19 ,20
These efforts seem to be paying off. In 2009, India's National Coverage Evaluation Survey indicated that the rate of initiation of breast feeding within 1 hour of birth had increased from 24.5% to 34% nationally.21 In 2011, a survey in the country's 100 poorest districts—home to over 20% of India's children—indicated that early initiation of breast feeding had increased from 20% in 2007 to 37% in 2011.22 Finally, a national survey in 2014 indicated that early initiation of breast feeding had increased from 24.5% in 2006 to 44.6% in 2014 (ie, a 1.8-fold increase) with an average annual rate of increase of 10.3%. Importantly, in the seven states with the highest burden of neonatal mortality, the combined rate of early initiation of breast feeding increased from 12.5% in 2006 to 34.4% in 2014 (ie, a 2.7-fold) with an average annual rate of increase of 21.8%.23 This evidence seems to indicate that focused strategies, effective capacity-building initiatives, strong partnerships, vibrant community-based action, and strategic mass media communication contributed to double/triple the rate of early initiation of breast feeding.
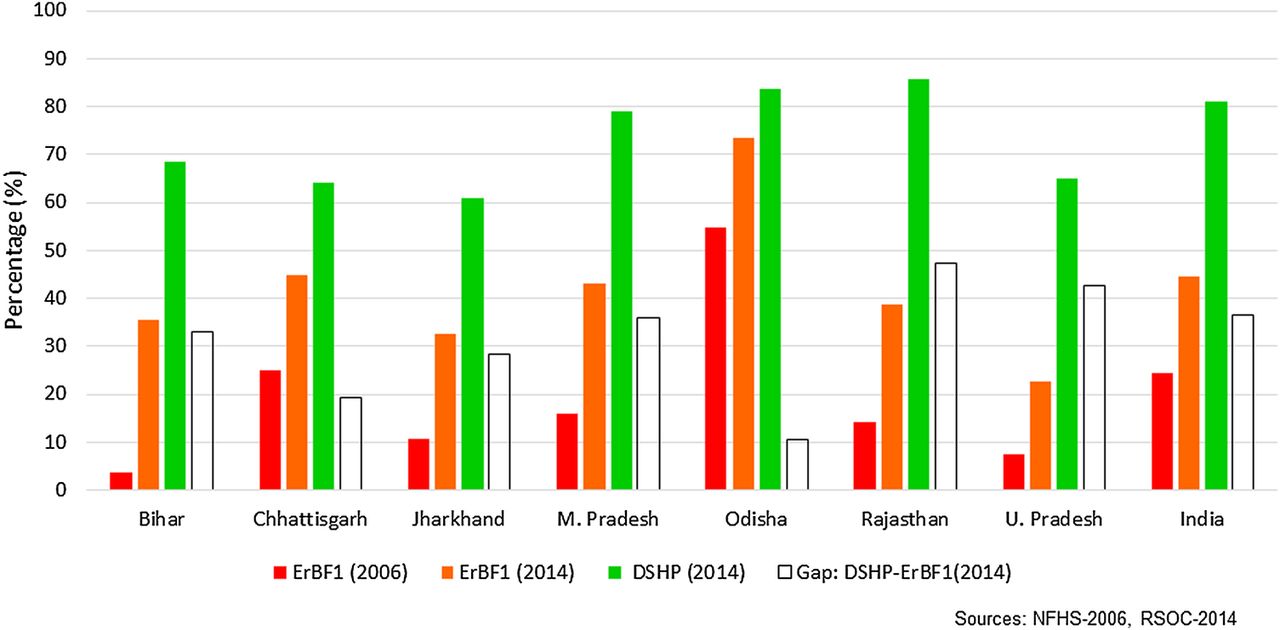
However, these data also indicate that room for further improvement still exists. The 2014 national survey shows that 81.1% of deliveries were attended by a skilled health provider, while only 44.6% of newborns were breast fed within 1 hour of birth (figure 1), indicating that rates of early initiation of breast feeding could almost double if all newborns delivered by a health provider were breast fed within 1 hour of birth. Recent meta-analyses of health system- and community-based studies worldwide indicate that improving individual counselling or group education, supporting immediate breast feeding at delivery, and training health staff in lactation management (three interventions included in the Baby Friendly Hospital Initiative) increased the likelihood of early initiation of breast feeding by at least 20%. In addition, community-based group counselling and home-based individual counselling focusing on infant feeding decision-making and preparation for breast feeding increased the likelihood of early initiation of breast feeding by 65% and 74%, respectively.24 ,25

{kind=link}
Early initiation of breast feeding within 1 hour of delivery (ErBF1), deliveries attended by a skilled health provider (DSHP), and gap between DSHP and ErBF1 in the seven states in India with the highest burden of neonatal mortality.
Breast feeding initiation can be particularly delayed for infants born by caesarean section. India's National Family Health Survey 2015 shows that, in states such as Andhra Pradesh and Telangana, where 92% of deliveries are attended by skilled health providers, high prevalences of births by caesarean section (40% in Andhra Pradesh and 58% in Telangana) are associated with low rates of early initiation of breast feeding (37% in Telangana and 40% in Andhra Pradesh). Furthermore, prospective cohort studies in India have shown that infants born by caesarean section were almost four times less likely to initiate breast feeding within 1 hour of birth than infants born by vaginal delivery.26 However, global evidence suggests that, in the presence of adequate support, a caesarean section is not necessarily a barrier to timely initiation of breast feeding.24
Therefore, there is an urgent need to continue to strengthen national and state policies, hospital and maternity practices, and the knowledge and skills of birth attendants—physicians, midwives and nurses—to support early initiation of breast feeding as a key component of essential newborn care. Janani Suraksha Yojna and Indira Gandhi Matriva Sahyog Yohana—India's conditional cash transfer programmes to protect women during pregnancy, delivery and lactation—need to step up their efforts to ensure that facility- and community-based health workers provide mothers and families with timely information and counselling to support early initiation of breast feeding. The guidelines of Janani Suraksha Yojna include the promotion of early initiation of breast feeding as one of the responsibilities of the accredited social health activist, the incentivised community-based worker under Janani Suraksha Yojna. Similarly, supporting early and exclusive breast feeding is one of the objectives of the Indira Gandhi Matriva Sahyog Yohana programme. Private providers, who deliver up to 50% of the newborns in states such as Andhra Pradesh and Gujarat, also have a major role to play in ensuring that their newborn care practices are aligned with national policy and guidance to support early initiation of breast feeding. Both public and private sector providers need to reach out to mothers, families and communities with one unequivocal message: early initiation of breast feeding saves lives.
Footnotes
Handling editor Seye Abimbola
Contributors VMA led data analysis and manuscript writing. GG, GS and RK contributed to data interpretation and manuscript writing.
Disclaimer The opinions expressed in this paper are those of the authors and do not necessarily represent an official position of the organisations with which they are affiliated.
Funding UNICEF Regional Office for South Asia for analysis and manuscript writing.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.